Introduction
- ??? ?? ??
- GCS 14 ???
- SBP <90 mmHg
- RR >29 or RR <10
Initial Evaluation and Resuscitation of the Injured Patient
Primary survey
Airway Management with Cervical Spine Protection
Airway obstruction
Airway injury
Breathing and Ventilation
????? shock? ??????, fluid ?? ??? tension pneumothorax, cardiac tamponade ??? ?? ???.
- Tension pneumothorax
- Open pneumothorax
- Massive air leak
- D/t injury to the tracheobronchial tree
- Large intrapleural collection of air or blood causees diffusely diminished or absent breath
- Flail chest with underlying pulmonary contusion
- Fracture of >3 contiguous ribs in >2 locations creates an isolated chest wall segment (flail segment) that moves paradoxically (opposite) to the rest of the rib cage during inspiration ? impairedg eneration of negative intrathoracic pressure.
- Typically, also contuses the underlying lung.
- Fracture-related pain causes respiratory splinting and atelectasis
- Tx: internal pneumatic stabilization: endotrachial intubation + MV

Circulation with Hemorrhage Control
- “Blood on the floor and 4 more”
- Chest: ~40% of the blood volume/hemithorax
- Abdomen: ~ the entire blood volume
- Pelvis: ~ the entire blood volume; blood loss often hidden within the retroperitoneum
- Thigh: ~1-2L/thigh
- Trauma series: cervical spine latera, chest AP, pelvic AP
Hemorrhagic shock
Massive hemothorax
Massive hemoperitoneum
Mechanically unstable pelvis fracture with bleeding
Extremity blood loss
Cardiogenic shock
Cardiac tamponade
Neurogenic shock
Disability and Exposure
Intracranial hemorrhage/mass lesion
Cervical spine injury
Shock Classification and Initial Fluid Resuscitation
Persistent Hypotension
Secondary survey
Mechanisms and patterns of injury
Regional assessment and special diagnostic tests
Head
Neck


- Neck injury
- Platysma ??? ???? ??? ???? ???? ?? ?? ??.
- ?? ??? ??? ??
- Zone II ??
- ?????? ???? zone I, III ??.
- Active bleeding?? ??? ??? ??.
- ?? ?? ??: ??? ???? ??? ?? ??? > ?? ???
- Cervical injury
- ?? ?? ??? ??? strict immobilization.
- Spontaneous respiration ??? ??
- Lateral C-spine X-ray ? ?? ??? orotracheal intubation (NO neck extension), ?? ??? nasotracheal intubation
- Apnea
- Tracheostomy: 8? ??? ??, laryngeal injury ?
- Cricothyroidotomy: ?? maxillofacial injury
- Orotracheal intubation : ? ?? ???? ??
Chest

Abdomen




Often, blunt splenic injury can be managed nonoperatively (eg, observation with serial hemoglobin measurement, embolization)
If negative or inconclusive FAST, consider CT or DPL.

- Bladder rupture
- Clinical findings
- Hematuria (~90%)
- Suprapubic tenderness
- Difficulty voiding
- Associated pelvic fracture (eg, widening of the pubic symphysis)
- Diagnosis
- Retrograde cystography with water-soluble contrast and then imaged (eg, CT scan)
- Management
- Surgical repair (continued efflux of urine through the defect prevents spontaneous healing)
- Clinical findings
Pelvis
General Principles of Management
Transfusion practices
Prophylactic measures
Operative approaches and exposure
- L-tube
- ?? ??? ??? ?? (?? ??? ???? cribriform plate ??), ??? ???? ?.
- Evisceraion
- ?? ??? ?? ?? ?? ? wet gauze? ?? ??, ?? ??? ??? ??? ??. ????? ??.
- Stabbing knife
- ? ??? ??? ?? ?? ??? ??? ? ???? ??? ? ? ???? ??.
- Foley
- ???? ??, ??? ??? ?? ? urethrogram? ????? suprapubic cystostomy? ??.
Damage control survey
Treatment of Specific Injuries
Head injuries
Cervical injuries
- Cervical collar
- ?? ??: ??? ???? ?? ??? ?? ?
Chest injuries
Blunt cardiac injury (BCI)
Arrhythmia ranging from asymptomatic (eg, PVCs) to fatal (eg, VFib)
ACS from coronary dissection or thrombosis
Myocardial dysfunction (“myocardial contusion”)
Ruptured valve, septum or ventricular wall
Cardiac tamponade
Require 24-48 hours of continuous cardiac monitoring d/t the risk of life-threatening arrhythmia.
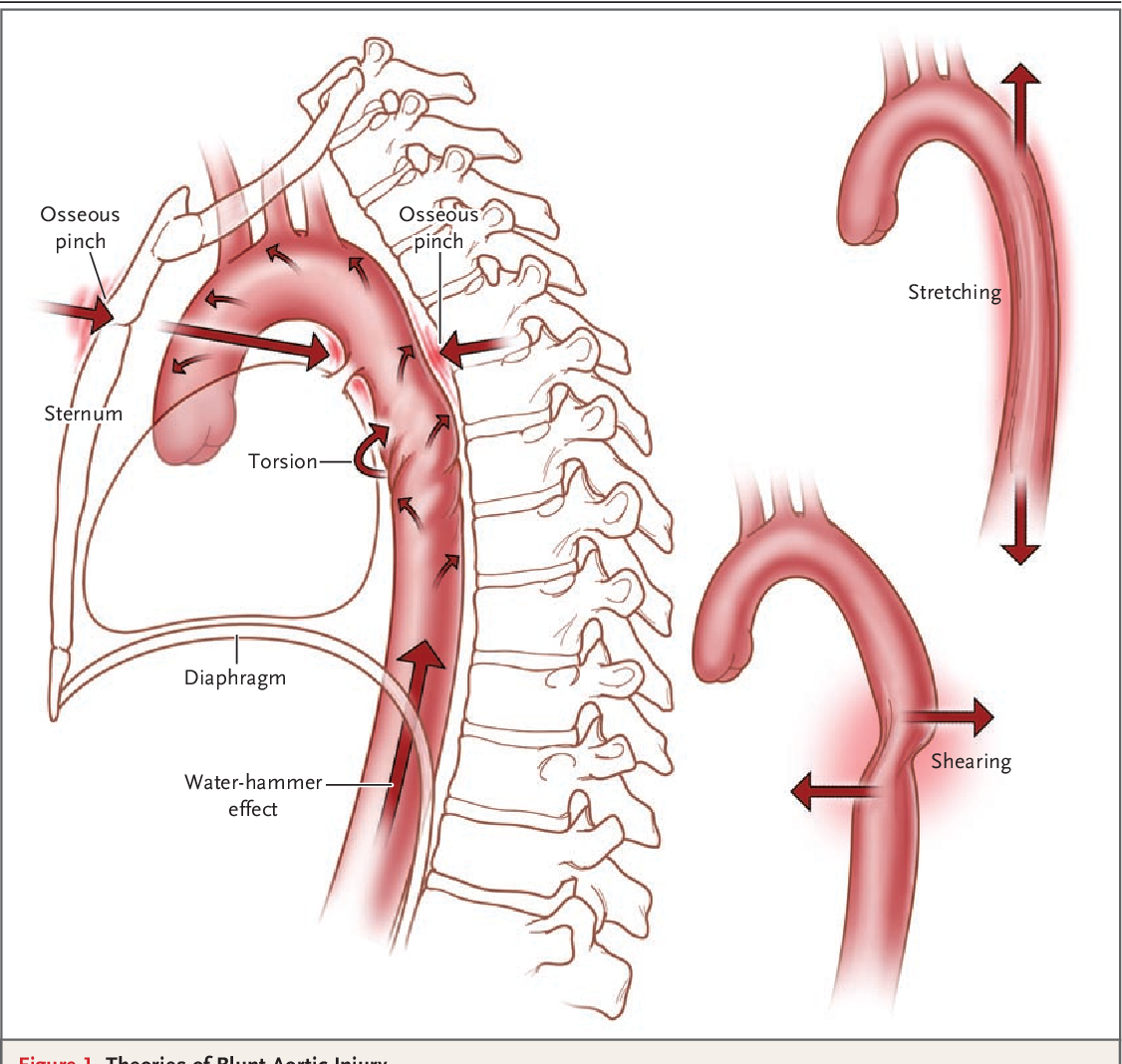
Blunt thoracic injury
Bruising and tenderness over sternum = blunt thoracic injury
Isthmus of thoracic aorta is most vulnerable location to deceleration injuries ? thoracic aortic aneurysm (widened mediastinum)
Dx: CT angiography
- Fractured ribs with intercostal vessel injury
- Pleuritic chest pain and exquisite chest wall tenderness to palpation
- Hemothorax
- Treated with tube thoracotomy, which is sufficient to resolve many cases
- If immediate chest tube output is >1,500 mL of blood, emergent surgical thoracotomy is indicated.
Penetrating chest trauma
- Cardiac tamponade
- Can be visualized by TTE
- Severe hypotension, tachycardia, elevated JVP, distended neck vein
- Treated with pericardiocentesis
- Hemothorax
- Tube thoracostomy
- Clamping is not recommended.
- Although it’s often sufficient to manage hemothorax, some patient (up to 15%) require emergenet thoracotomy for extreme bleeding.
- Emergent thoracotomy
- Initial bloody output > 1,500mL
- Persistent hemorrhage > 200mL/hr for >2 hours or continuous need for blood transfusion to maintain hemodynamic stability.
- Tube thoracostomy
Abdominal injuries
Blunt abdominal trauma (BAT)
Spleen
- m/c injured organ. Often associated with fractured left ribs 9-11
- Not visible on plain abdominal X-ray ? CT scan with IV contrast.
- Hemodynamically stable
- Conservative treatment
- Hemodynamically unstable
- Surgical resection.
- Give vaccines 2 weeks later if spleen is removed
Liver
- Hemodynamically stable
- Hemodynamically unstable
- Surgical repair.
Kidney
Duodenum
- Duodenal laceration
- Common in handle bar injury.
- Epigastric pain + bilious emesis
- Retroperitoneal free air
- Susceptible d/t location from vertebral column, multiple attachments (eg, hepatoduodenal ligament, ligament of Treitz)
- Treated with surgical repair.
- Duodenal hematoma
- Hemodynamically stable patient can be managed conservatively as they usually resolve spontaneously within 3�4 weeks.
- L-tube + TPN
Pancreas
- Also common in children with handlebar injuries
- Epigastric pain + nonbilious emesis
- Nausea accompanied by a low-grade fever and a large abdominal fluid collection.
- Grade I, II
- ?? ?? ?? ?? ??? ??? ??
- ?? ?? ??, PCD drainage.
- Grade III (distal injury)
- Distal pancreatectomy
- Grade IV, V (proximal injury)
- Whipple’s op.

Diagphragm
Penetrating abdominal trauma
- Colon
- ?? 4-6?? ?: primary closure
- Dirty & delayed colon injury, rectum injury: colostomy
Pelvic fracture hemorrhage control


- Hemodynamically stable
- ICU?? ?? ??
- Hemodynamically unstable
- ?? ???? (eg, Pelvic binder)
- Arterial embolization
Extremity vascular injuries, fractures, and compartment syndromes
- Vascular assessment
- Focus on identifying hard signs of injury, including:
- Observed pulsatile bleeding
- Presence of a bruit or thrill over the injury
- Expanding hematoma
- Signs of distal ischemia (eg, absent pulses, cool extremities)
- Predictive of the need for urgent surgical repair and warrant immediate exploration.
- If the area of damage is unclear, arteriography can be performed intraoperatively to clarify anatomy.
- Focus on identifying hard signs of injury, including:
- If hard signs are absent, further evalaution for soft signs, including:
- History of hemorrhage
- Diminished pulses
- Bony injury
- Neurologic abnormality
- If present, these signs indicate additional testing such as the injured extremity index (similar to ABI)
- If the index is abnormal (<0.9), considered for CT scan or conventional arteriography and surgery in conjunction with management of other injuries (eg, bony damage)
- Duplex Dppler ultrasonography can be an acceptable alternative to angiography
Open fracture
?? 5-7? ? ????, ??? ?????? ??.
Surgical Intensive Care Management
Postinjury resuscitation
Abdominal compartment syndrome

Etiology
- Intra-abdominal hypertension
- d/t intra-abdominal injury
- Major intraabdominal surgery
- Inflammatory condition that can cause abdominal swelling from visceral edema, intraabdominal third spacing of fluids, and ileus.
- Acute pancreatitis
- Splanchnic reperfusion after massive resuscitation.
- Intraabdominal fluid collections (eg, bleeding, ascites)
Clinical manifestations
- Tense, distended abdomen
- ?Ventilatory requirements (d/t diaphragmatic elevation, ?intrathoracic pressure)
- ?CVP (d/t venous compression but ?venous return & cardiac output)
- ?Urine output (?intraabodminal organ perfusion)
Diagnosis
- ???? ??
- ????? ??. 25cmH2O ???? ?? ?? ??.
Management
- Temporizing measures
- Avoid over-resuscitation with fluids
- ?Intraabdominal volume (eg, NG tube, drain fluid collections)
- ?Abdominal wall compliance (eg, sedation, paralysis)
- Definitive management: surgical decompression
Leave a Reply