Epidemiology and risk factors
- The m/c risk factor is obesity.
- Protective factors
- Oral contraceptives (E+P)
- Tobacco use
- Stimulating estrogen metabolism in the liver and decreasing serum estrogen levels.
## Endometrial biopsy indications
- Age ≥45
- Abnormal uterine bleeding
- Postmenopausal bleeding
- Age <45
- Abnormal uterine bleeding PLUS:
- Unopposed estrogen (obesity, anovulation)
- Failed medical management
- Lynch syndrome (HNPCC)
- Abnormal uterine bleeding PLUS:
- Atypical glandular cells on Pap.
- Age <35: common, benign especially during the menstrual cycle
- Age ?35: need colposcopy + ECC + biopsy
Endometrial hyperplasia
Risk factor
- Unopposed Estrogen
- Nullipara / late menopause
- PCOS
- Granulosa-theca cell tumor
- OCS(single)
- tamoxifen / raloxifen
- Obesity
Diagnosis
???: ?? ??, ????, ????
???: ? ?? (??? 5-10%)
- USG
- Premenopuase 14mm
- After menopause 4mm
- Aspiration Bx, Hysteroscopy, D&C
C14 Benign Diseases of the Female Reproductive Tract
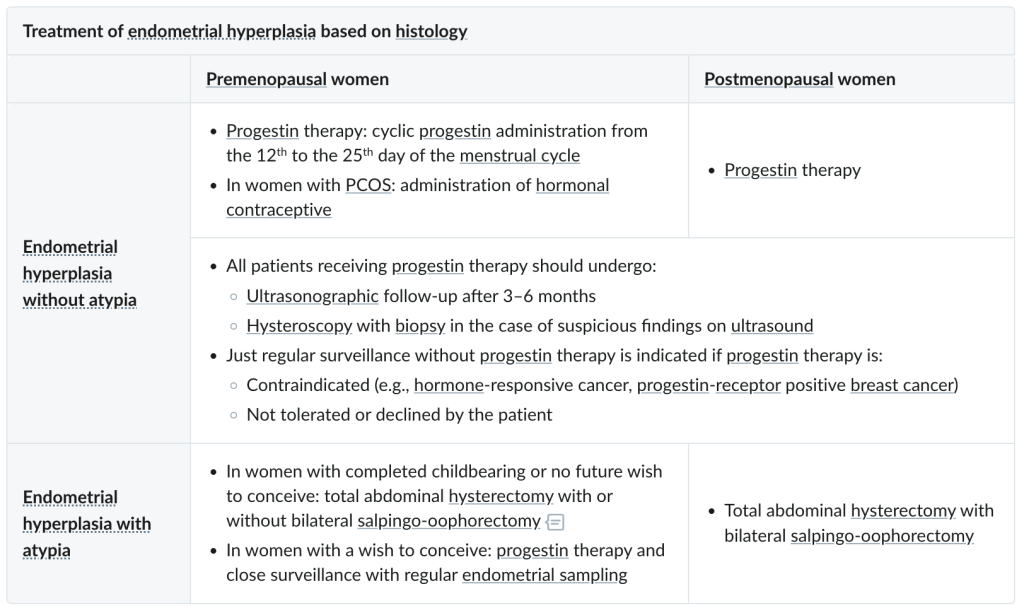
Treatment
Progestin Tx? 2-3???. ?? 1?? ? Bx ????.
| Premenopausal | Postmenopausal | |
| NO atypia | Cyclic low P | Cyclic low P |
| WITH atypia | Continuous high P TAH c BSO | TAH c BSO |
- If Cyclic low P fails, Cont. low P
- Continuous high P: 3month f/u Bx/TVUSG.
Endometrial cancer
Similar risk factors with hyperplasia. + HNPCC – POF
| Type | Type I (75%) | Type II (25%) |
| Cause | E dependent | E independent, p53 mutation is common. |
| Arises from? | Endometrial hyperplasia | Atrophic hyperplasia |
| Histology | Endometrioid | Papillary structures with psammoma body |
| Age | Younger | Older |
| Prognosis | Favorable | Poor |
Clinical presentation
???? ? ?? (90%), ?? ?? ??? DDx: ?? ?? ?? – m/c
Diagnosis
Physical exam: Pelvic exam, US;?? ??? 4mm??? ??
Screening test: ??. ???? Pap, cytology, USG(???? ??? ??? ?), CA125
US: ??? 14mm, ?? ? 4mm
Aspiration Bx
Hysteroscopy
D&C
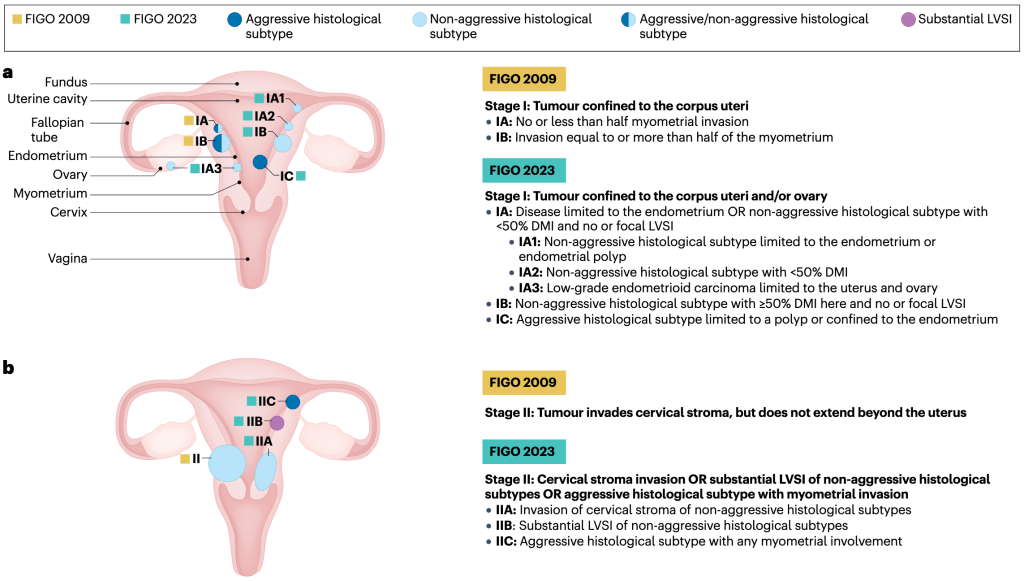
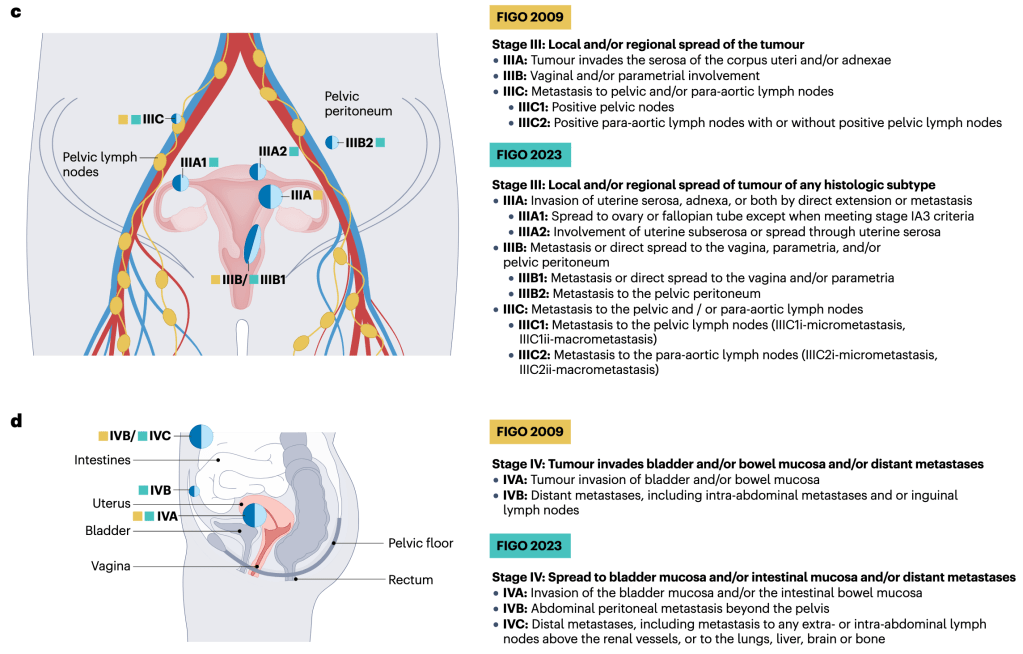
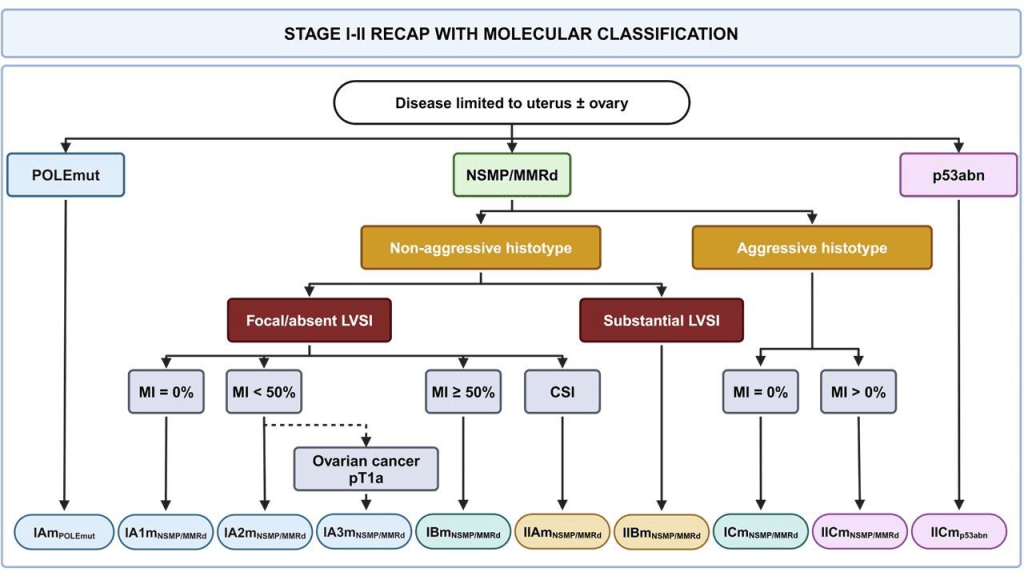
Staging process
Surgical Flow
Peritoneal fluid cytology ? abdomen/pelvis explore ? TAH&BSO ? uterine specimen eval. ? suspicious LN sampling
Staging
Surgically, after TAH+BSO.
Histology
Bad: nonsquamous or nonmorular solid growth pattern
G1: ~5% / G2: 5~50% / G3: 50%~
Molecular profiling
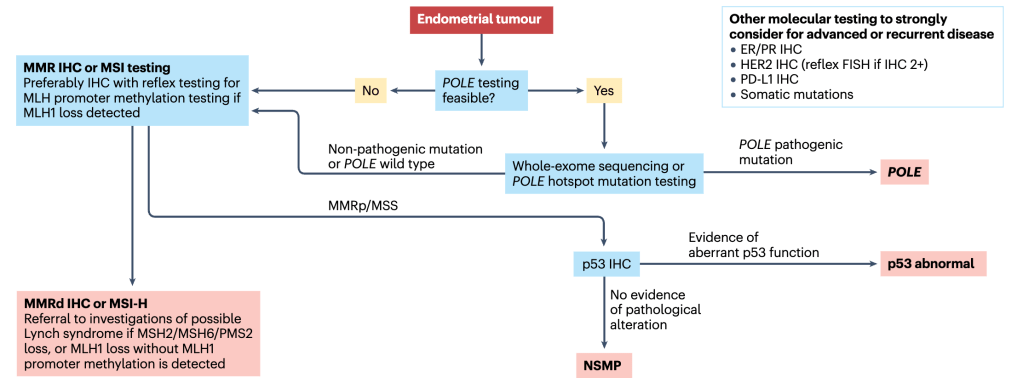
cancer. MMR, mismatch repair; MMRd, mismatch repair-deficient; MMRp, mismatch
repair-proficient; MSI, microsatellite instability; MSI-H, microsatellite instability-
high; MSS, microsatellite stable; NSMP, no specific molecular profile; POLE, DNA
polymerase ε; PR, progesterone receptor.
Treatment
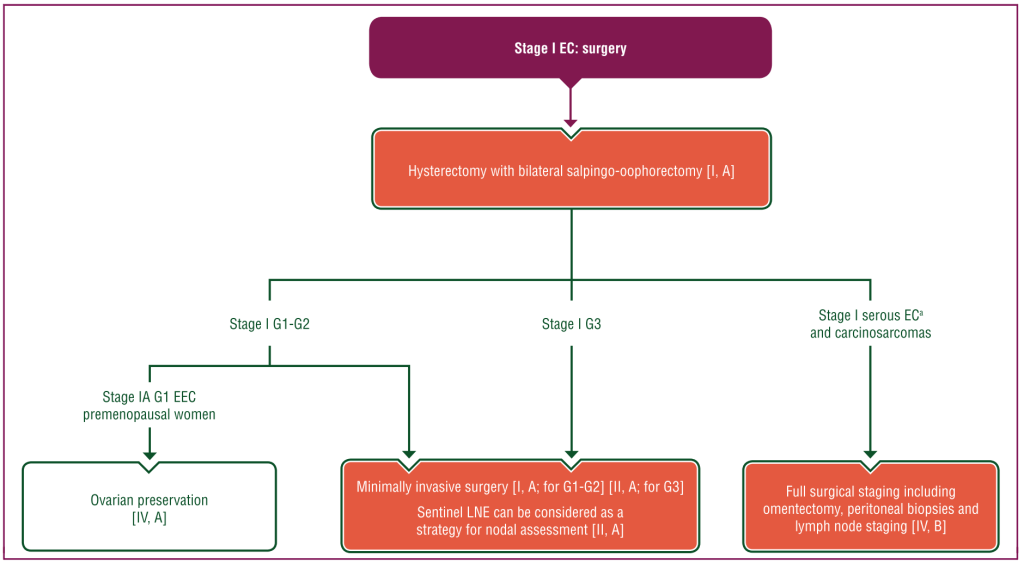
Pelvic, para-aortic LND Indication
- Histology
- Non-endometrioid (serous, clear, squamous)
- Grade 2-3 endometrioid
- ???? 1/2 ?? ?? (stage IB ??)
- ?? ?? >2cm
- ??? 2cm ??? ?? pelvic,
- Pelvic?? ??? para-aortic??.
- Isthmus-cervix extension
- ?? ? ?? ??
Recurrence risk
- Risk factors
- 60? ??
- LVSI (+)
- Size >2cm
- Uterine ?? ??
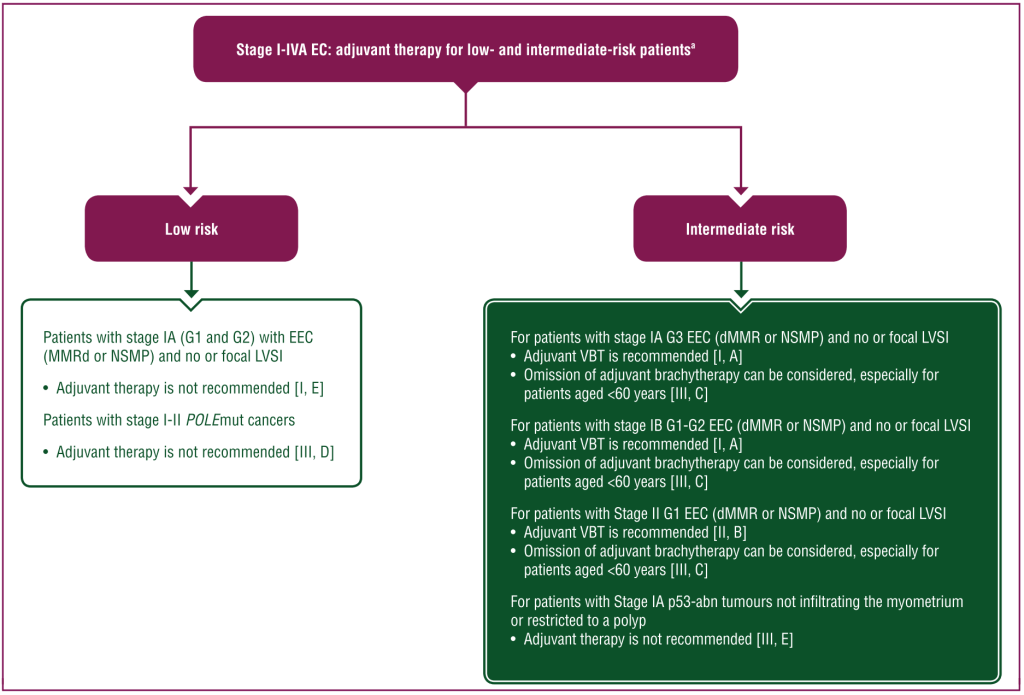
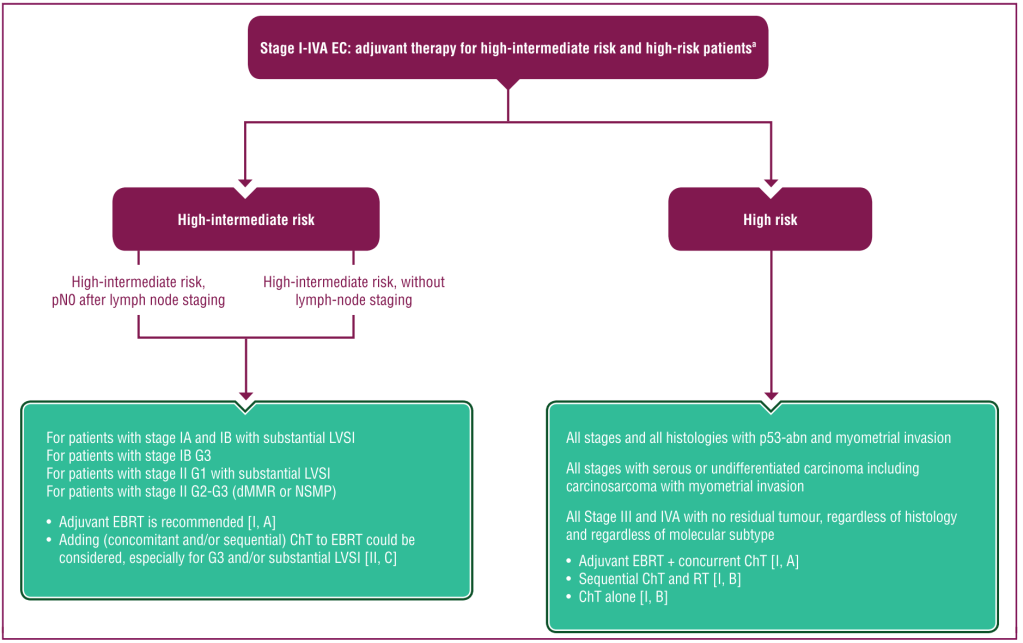
- Risk factor ?? ?? RTx or CTx ??? ??.
- RTx
- Stage IA G2~: vaginal brachytherapy (local)
- Stage IA G3~: pelvic RTx (external)
- + Extended field RTx, whole abdomen RTx, Etc.
- CTx
surgical staging ?
RTx
IB G3 RF+ ??? ??? RTx ?? ??.
Vaginal vault < External pelvic < Extended field < Whole abdomen
CTx
IB G3 RF+, II G3 ??? CTx ?? ? ??. III?? ??? ????.
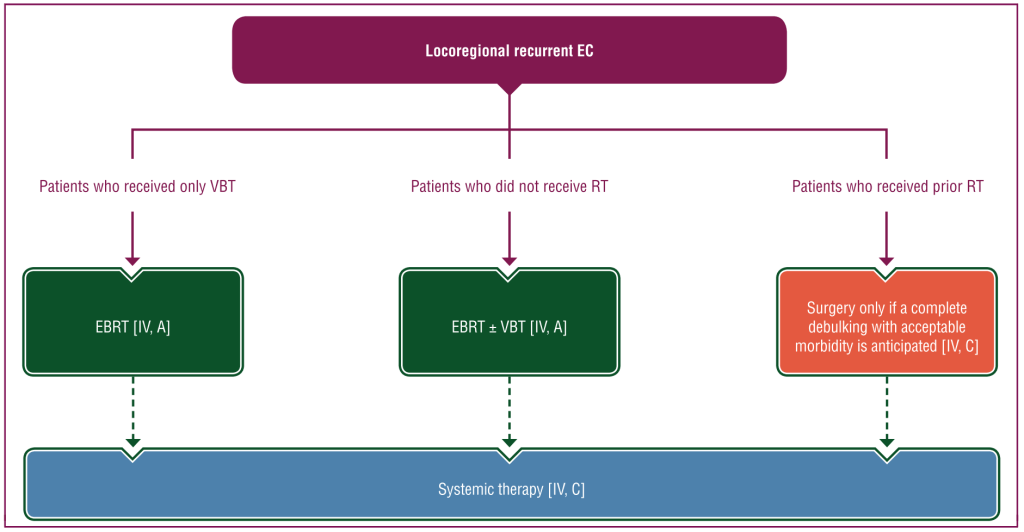
???
1/4??, ??? 2? ??. Vagina>pelvis>lung>LN
??? ? ???. Palliative, RTx ?????? ??????
??? ? ???? ?? ??? E ??? controversial
??? ????? – IB?? ??? RTx. ?? ?? ????? ????.
Uterine sarcoma
Risk factors
Pelvic radiation, tamoxifen use, postmenopausal patients
Presentation
Abnormal/postmenopausal bleeding
Pelvic paian or pressure
Uteraine mass
Diagnosis
Ultrasound +/- additional imaging
Endometrial biopsy
Histopathology of surgical specimen
Leiomyosarcoma
Malignant proliferation of smooth muscle arising from the myometrium(usually seen in postmenopausal women).
Arises de novo; leiomyosarcomas do not arise from leiomyomas.
Gross exam often shows a single lesion with areas of necrosis and hemorrhage; histological features include necrosis, mitotic activity, and cellular atypia.