Cell with hypoxia can cope with the low oxygen tension in two ways:
→ Increasing delivery of oxygen or Adapting to the low oxygen level
1 Hypoxia-inducible factors (HIFs)
- Transcription factors that facilitate both oxygen delivery & adaptation to oxygen deprivation by regulating the expression of genes (glucose uptake, metabolism, angiogenesis, erythropoiesis, cell proliferation, apoptosis)
- Composition: heterodimer, α-subunit (oxygen sensitive), β-subunit (constitutively expressed)
- α-subunit possesses oxygen dependent degradation domain (ODD)
ODD regulates HIF-1α degradation by the ubiquitin-proteasome pathway
- β-subunit: known as the aryl hydrocarbon receptor nuclear translator (ARNT)
- α-subunit possesses oxygen dependent degradation domain (ODD)
- Three categories: HIF-1, HIF-2, HIF-3
- HIF-1
- Global regulator of hypoxia-inducible gene expression – ubiquitously expressed & inducing the expression of most hypoxia-inducible gene
- Bound an 18-nucleotide fragment of the erythropoietin enhancer → hypoxic activation of erythropoietin
- HIF-2: Expression of HIF-2α is restricted to endothelial cells, glial cells, pneumocytes type II, cardiomyocytes, fibroblasts of the kidney, interstitial cells of the pancreas/duodenum/hepatocytes
- HIF-3: The role in the hypoxic regulation of target gene expression in vivo is not understood
Oxygen-dependent regulation of hypoxia-inducible factor

The transcriptional activity of HIF is regulated through changes in protein stability and through recruitment of transactivation coactivators (Fig 26.1)
Regulation through hydroxylation with ODD, 4-prolyl hydroxylase (PHD)
- Under normoxic conditions:
Hydroxylation of HIF-α by PHD → binding to the von Hippel-Lindau (VHL) tumor suppressor protein → destruction by the proteasome - Under hypoxic conditions:
shortage of oxygen → Hydroxylation↓ of HIF-α → not recognized by VHL protein → HIF-α escapes the destruction by proteasome → stabilization of HIF-α → dimerization with HIF-β → binds to a core sequence of 5’-RCGTG-3’ → initiating gene transcription
Regulation at the level of recruitment of co-activators
Regulation through asparaginyl hydroxylase factor inhibiting HIF (FIH)
- FIH under normoxic condition → Hydroxylation of C-terminal transactivation domain(asparagine residue 803) → preventing interaction between HIF and p300 → preventing gene transcription
Cancer mutations that activate hypoxia-inducible factor
Mutation of VHL → HIF can be activated under normoxic condition → increased target expression irrespective of oxygen status
Examples:
- Germ line mutations in VHL → familial tumor syndrome, development of highly vascularized neoplasm (hemangioblastoma of retina, CNS, RCC, endocrine and exocrine pancreas tumor, pheochromocytomas)
- Sporadic VHL mutation is found in most sporadic RCC, hemangioblastomas
Important roles of hypoxia-inducible factor in tumors
HIFs activation: key steps for tumor cells to adapt and survive, promoting tumor progression, angiogenesis, metabolism and metastasis
Tumor Angiogenesis
- Normal tissues keep a balance between proangiogenic & antiangiogenic factors
- Tumor: proangiogenic factors↑
Vascular endothelial growth factor-A (VEGF-A) induced by HIF: most critical, expressed in many tumors of human.
Tumor metabolism
- Warburg effect : shifting glucose metabolism from oxidative to glycolytic pathway in cancer cell
- HIF-1 regulates the expression of genes involved in glycolytic metabolism (glucose transporters, glycolytic enzyme, lactate production and pyruvate metabolism)
Tumor metastasis
- HIF activation correlates with metastasis
- Promotes the transcriptional regulation of key factors that govern cell adhesion, extracellular matrix formation, cell migration (Metalloproteinases, lysyl oxidase, CXCR4)
HIF and radiotherapy
Important role in determining tumor response to RT & tumor regrowth
Radiation results in a reoxygenation-dependent increase in HIF-1 activity
- Vasculature resistance ↑
- Reoxygenation due to RT → reactive oxygen species → HIF-1 stabilization & enhanced translation of HIF target, tumor vasculature radioresistance↑
- Radiosensitization due to HIF-1: induction of apoptosis due to HIF-1
- Overall, HIF-1 stabilization promotes radio-resistance
- Recruitment of BM-derived cells which promote vasculature of tumor
2 Unfolded protein response(UPR)
Prolonged periods of hypoxia can activate non-HIF signaling such as UPR
UPR: cellular response induced by the accumulation of unfolded proteins in the endoplasmic reticulum (ER) in order to deal with the problems associated with the accumulation of misfolded proteins
Accumulation of misfolded proteins in ER → ER stress↑ → activation of ER stress sensor (inositol-requiring kinase, protein kinase-like endoplasmic reticulum kinase) → transient inhibition of protein translation, induction of chaperone proteins to assist in folding, trafficking, secretion of accumulated proteins
3 Radiosensitizing hypoxic cells
Methods suggested to overcome the radioresistance induced by hypoxia: hyperbaric oxygen chambers, high LET radiation, chemical radiosensitizers, hypoxic cytotoxins
Hyperbaric oxygen
Chambers filled with pure oxygen raised to a pressure of three atmospheres
- Limitation: time↑ & effort↑, Patient compliance d/t claustrophobia, risk of fire → fell into disuse
- Multicenter trials performed by the Medical Research Council in the UK: a significant benefit in local control & survival for cervical carcinoma, advanced H&N cancer, but also an increase in late toxicities
Breathing oxygen rather than air
- But pure oxygen induces vasoconstrictions
- Carbogen: oxygen + 5 % carbon dioxide
Improving the oxygen supply to tumors
A study in Princess Margaret Hospital: a blood transfusion before RT led to a significant improvement in local control for uterine cervical carcinoma
Smoking: decrease tumor oxygenation → patients should stop smoking during RT
Hypoxic cells radiosensitizers
Oxygen substitutes diffuse into poorly vascularized areas of tumors and desired effect by chemical mean
Requirements for a clinically useful hypoxic cell sensitizer
- Selectively sensitize hypoxic cells at a concentration resulting in acceptable toxicity
- Chemical stable, not rapidly metabolized by cells
- Highly soluble in water or lipid, be capable of diffusing a considerable distance
- Effective at the relatively low daily doses of a few grays
Misonidazole (2-nitroimidazole, Fig 26.4)
- Very effective radiosensitizing substance in vitro & in animal experiment
- Enhancement ratio in mouse, single fraction RT after administration of misonidazole: 1.8
- In clinical trials, disappointing results.
- No significant results from 20 or so randomized prospective controlled trials by RTOG
- The only trial that show a clear advantage: Danish H&N cancer trial
Benefit in only the subgroup with males with high hemoglobin levels and cancer of the pharynx: double tumor control in 3 yrs - Dose-limiting toxicities: peripheral nerve toxicity progressed to central nerve toxicity. → prevented use the drug at adequate dose levels through multifraction → a probable reason of disappoint results in many clinical trials
Etanidazole and Nimorazole
- Etanidzole (2-nitroimidazole)
- equal sensitizing effect as misonidazole,
- shorter half-life → less toxic → dose can be increased
But poor penetration into nerve tissue & BBB - No benefit in the RTOG controlled clinical trial and the multicenter trial in Europe
- Nimorazole (5-nitroimidazole)
- Less effective in sensitizing, but much less toxic than misonidazole, etanidazole
- In a Danish H&N trial, a significant improvement in both locoregional control and survival for supraglottic and pharyngeal carcinoma
Overgaard’s meta-analysis of clinical trials addressing the problem of hypoxia
10,602 patients treated in 82 randomized clinical trials, including hyperbaric oxygen, chemical sensitizers, carbogen breathing, blood transfusions
Overall, local tumor control was improved by 4.6%, survival by 2.8%, & complication rate increased by only 0.6%, which was not statistically significant
Greatest benefit showed in H&N cancer,
Marginal effect in most adenocarcinoma, important in SqCC
Nicotinamide and carbogen breathing
Nicotinamide: vitamin B3 analogue, prevents transient fluctuations in tumor blood flow that lead to acute hypoxia
ARCON (accelerated hyperfractionation radiotherapy, carbogen, nicotinamide) trial
- Janssens et al. JCO 2012;30:1777-83
- Accelerated, to overcome proliferation
- Hyperfractionated, to spare late-responding tissues
- Carbogen breathing, to overcome chronic hypoxia
- Nicotinamide → overcome acute hypoxia
- No difference in 5yr LC, larynx preservation rates, overall survival, toxicity
- Significantly increased regional control, specifically observed in patients with hypoxic tumors
- Conclusion: benefit for patients with hypoxic tumor
4 Hypoxic cytotoxins
To develop drugs that selectively kill hypoxic cells
Drugs that are reduced preferentially to cytotoxic species in the hypoxic regions of tumors
5 classes of agent
- Quinone antibiotics
- Nitroaromatic compounds
- Benzotriazine di-N-oxides
- Nitrobenzdimide modified nitrogen mustard
- 2–nitroimidazole attached to dibromo isophosphoramide
Mitomycin C
- Active against hypoxic cells in a wide range of tumors
- Hypoxic/oxic cytotoxicity ratio is quite small
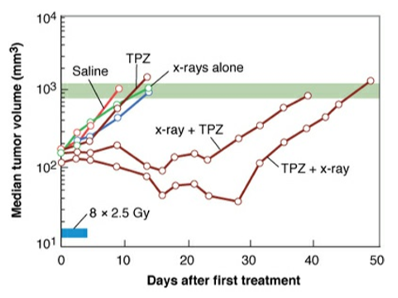
Tirapazamine
- Hypoxic/oxic cytotoxicity ratio: about 100 for Chinese hamster cells, but, about 20 for cells in human origin
- RT+tirapazamine: Significant growth delay in mouse carcinoma (Fig 26.9)
Clinical trials with tirapazamine and new bioreductive drugs
Little clinical trials about tirapazamine and radiotherapy, due to side effect (nausea, severe muscle cramping)
- TROG 02.02, HeadSTART
- Advanced H&N SqCC, phase III trials
- Tirapazamine, cisplatin, radiotherapy vs. cisplatin, radiotherapy
- No difference in either failure-free survival, time to locoregional progression or quality of life
→ need to stratify patients according to hypoxic proportion
Other drugs
- Tricyclic triazine-di-N-oxides(TTOs): superior selective cytotoxic to tirapazamine in vivo
- Hypoxia-activated DNA crosslinking agent (PR-104), hypoxia-activated dibromoisophoramide mustard (TH-302)
5 Targeting tumor metabolism to kill hypoxic cells
Altered metabolism: mitochondrial metabolism↓ & glycolysis↑ → tumor cells conserve oxygen and can survive under hypoxic condition
Denko et al: HIF-1-pyruvate dehydrogenase kinase 1 (PDK1) axis as major regulators for this shift
HIF-1 induction of PDK1 → inactivation of pyruvate dehydrogenase
Inhibition of PDK1 → oxygen consumption↑ → tumor hypoxia increases
Dichloroacetate (DCA): a safe inhibitor of PDKs
Increase mitochondrial metabolism → reprogram tumor metabolism to be more oxidative