188 Dermatology Assessment
Normal skin
Harlequine color change
Mongolian spot
Salmon patch
Erythema toxicum
Nevus flammeous (=portwine stain)
Mottling
Milia
- Salmon patch (40%)
- ?? ???? ?????, ???? salmon patch ? 50%? ??.
- Erythema toxicum (50%)
- ?/??? ?? ??. ??? ??.
- Atopy? 2-3?? ???. ??? ???x
- Nevus flammeous (=portwine stain, 0.3%)
- ?? ??? ???? ???? ??.
- ?? ????? ????
- -> Pulsed dye laser (PDL)
- Cosmetic camouflage
189 Acne Vulgaris
190 Atopic Dermatitis
191 Contact Dermatitis
192 Seborrheic Dermatitis
193 Pigmented Lesions
Congenital dermal melanocytosis (CDM, “Mongolian spots”)

Benign, flat, blue-gray patches that are usually found in infants over the lower back and buttocks.
Most infants of African, Asian, and Hispanic ethnicity have CDM at birth. Slowly fading, resolve by the age of 10.
No treatment is required as the hyperpigmentation usually fades spontaneously during the first decade of life.
# Congenital melanocytic nevus (CMN)

- Within the first few months of life and are usually solitary, hyperpigmented lesions with increased density of overlying dark, coarse hair. Abdomen, buttock
- Benign, can grow during infancy and appear as heterogeneously pigmented and raised.
- Risk of transformation to melanoma
- Large (~5%) lesions: often removed surgically to reduce risk.
- Small or medium (<1%) lesions: exceedingly rare.
194 Vascular Anomalies
Infantile hemangioma
(=strawberry naevi)

- Solitary lesion at birth, red, painless papule/macule, head or neck.
- Rapid grwoth followed by spontaneous resolution by the age of 5 yrs.
- Management: BB, Steroid, PDL
195 Erythema Multiforme, Reactive Infectious Mucocutaneous Eruption, SJS/TEN
196 Cutaneous Infestations
Cystic hygroma
???~?? mass, diffuse. Associated with Turner syndrome
venous drain ?? – ?? ? MRI? extent ????.
Sclerosing agent+?????
Torticollis
- Etiology
- Birth trauma (eg, breech delivery)
- Malposition of the head in utero (eg, d/t fetal macrosomia or oligohydramnios)
- ? SCM injury and fibrosis
- May have additional musculoskeletal anomalies
- Hip dysplasia
- Metatarsus adductus (ie, adduction of the forefoot)
- Talipes equinovarus (ie, clubfoot)
2-4? ? ???.
1-6??? ???? ??? ??? ?? ??? ??? ?? ? (positional plagiocephaly)
12???? ??? ????? ???? ?? ?????.
C667 Cutaneous defects
Skin dimples
Sacral dimples
Cutaneous stigmata of occult spinal cord malformations
Redundant skin
Amniotic contriction bands
Preauricular sinuses and pits
Accessory tragi
Branchial cleft and thyroglossal cysts and sinuses
Brachial cleft cyst
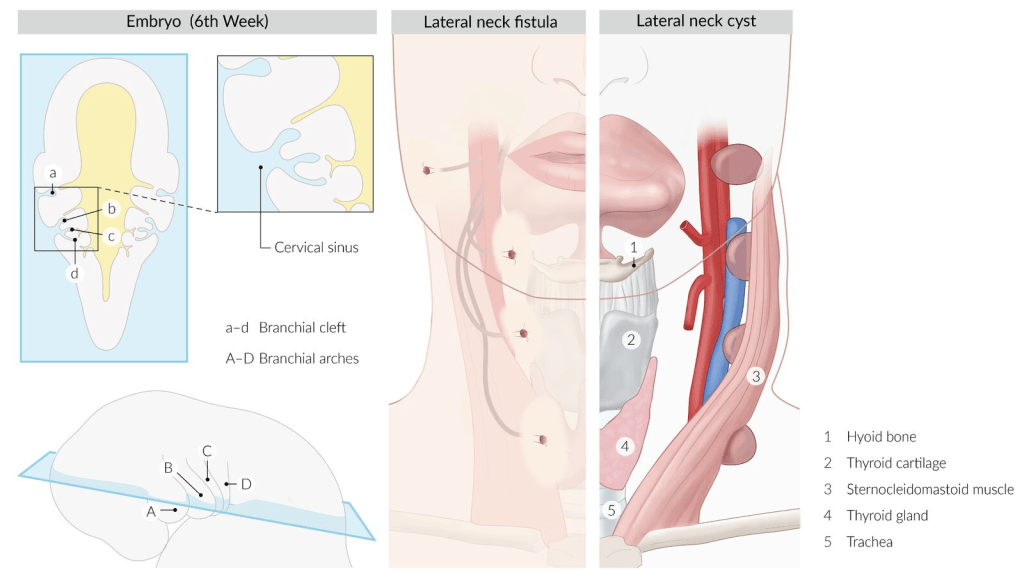
- ? ??~?? mass.
- Often detected when it becomes secondarily infected after an URI
- Erythema, tenderness, and sometimes drainage of fluid from a sinus tract.
- ??? ?? or ??? ??
Thyroglossal cyst

Unlike branchial cysts, a thyroglossal duct cyst often appears after an URI
2nd remnant-m/c
SCM ?? 1/3??? ?
Clinical features
- Located in the midline of the neck
- Move upwards during swallowing
Evaluation
- Ultrasound
- ??? ???? ? ???, ?? ???? ???? cyst ??? ?? ?? ??.
- As well as to confirm that surgical excision of the cyst would not result in postoperative hypothyroidism
- TFT
- May be normal even if the ectopic thyroid tissue is the only functioning tissue.
- But it may be useful if the thyroid gland has an abnormal appearance or is not visualized on ultrasound.
Scintigraphy- It is unnecessary to perform if the imaging method of choice reveals normal thyroid architecture and thyroid function testing is normal.
- Additionally, exposing children to radionucleotide material should be avoided, if possible.
Sistrunk op.: hyoid ???? ?? ??
Supernumerary nipples
C673 Vesiculobullous Disorders
C673.1 Erythema Multiforme
C673.2 Stevens-Johnson Syndrome
C673.3 Toxic Epidermal Necrolysis
C673.4 Mechanobullous Disorders
Epidermolysis Bullosa
Inherited disorders characterized by epithelial fragility triggered by minor trauma.
Caused by mutations of proteins involved in intraepidermal and dermoepidermal adhesion complexes in the basement membrane zone.
Diagnosis: biopsy of a fresh blister for immunofluorescence microscopy
? Following 4 types.
Epidermolysis Bullosa Simplex
In children and young adults with friction-induced blisters at the palms and soles and other exposed areas.
The lesions typically heal with no residual scarring, although patients may have chronic thickening of the skin of the feet.
Infants: oral blisters with bottle-feeding
Junctional Epidermolysis Bullosa
Dystrophic Epidermolysis Bullosa
Kindler Syndrome
C673.5 Pemphigus
C673.6 Dermatitis Herpetiformis
C673.7 Linear Immunoglobulin A Dermatosis (Chronic Bullous Dermatosis of Childhood)
C674 Eczematous Disorders
C675 Photosensitivity
C676 Diseases of the Epidermis
C677 Disorders of Keratinization
Ichthyosis vulgaris
- Pathogenesis
- Mutations of the filaggrin gene (AD)
- Also seen in atopic eczema. Family history of eczema.
- Epidermal hyperplasia, defective keratinocyte desquamation
- Accumulation of dry, scaly skin with loss of normal barrier function.
- Mutations of the filaggrin gene (AD)
- Clinical lpresentation
- Usually between 3 and 12 months of age
- ??? ????(palmar hyperlinearity), ???, ????? ??? – rudnfdp tlagowla.
- Treatment
- ?? ?? ??? ?? ??! ?? ???? ?? ???
- Skin moisturizers (eg, creams containing urea or pantheon)
- Topical retinoids
- Prognosis
- Good; lesions disappear during adolescence
X-linked ichthyosis
Occurs almost exclusively in boys and causes dry, scaly lesions to appear in early childhood, with sparing of the antecubital fossa and popliteal fossa.
However, the scales in X-linked ichthyosis would be larger and brown in color, unlike the fine, light gray scales seen in ichthyosis vulgaris.
Also, the palms and soles would not be affected, and hyperkeratosis would be visible on the neck and the lateral aspects of the trunk.
C678 Diseases of the Dermis
Keloid
Striae cutis distensae (stretch marks)
Corticosteroid-induced atrophy
Granuloma annulare
Necrobiosis lipoidica
Lichen sclerosus
Morphea
Scleredema (scleredema adultorum, scleredema of buschke)
Lipoid proteinosis (urbach-wiethe disease, hyalinosis cutis et mucosae)
Macular atrophy (anetoderma)
Cutis laxa (dermatomegaly, generalized elastolysis)
Ehlers-danlos syndrome
Inheritance and severity vary (can be AD or AR).
Hyper-extensible skin, hypermobile joints, and tendency to bleed.
S3 The skeletal dysplasias
C682 Disorders of Hair
Traumatic alopecia (traction alopecia, hair pulling, trichotillomania)
Traction alopecia
Hair pulling
Trichotillomania
Alopecia areata ??? ???
Congenital diffuse hair loss
Menkes kinky hair syndrome (Trichopoliodystrophy)
XR connective tissue disease caused by impaired copper absorption d/t defective Menkes protein (ATP7A)
-> ? Activity of lysyl oxidase -> defective collagen -> brittle, ?kinky? hair, growth retardation, and hypotonia
C685 Cutaneous Bacterial Infections
Staphylococcal infections
https://hsnowhome.wpcomstaging.com/2020/03/18/c142-staphylococcal-infections
Impetigo contagiosa
- S.aureus? ???, GAS? ????
- Erythema -> vesicle -> seropurulent fluid -> rupture ? ???? ?? (crust) ??
- ?? ? ?? ?? ???? ?? (?, ???? ??? ??)
Staphylococcal scalded skin syndrome; SSSS
Wart (Verruca)
Molluscum contagiosum

Trunk, intertriginous areas (eg, axillae), face (including eyelids)
? Reassurance. Self-resolve within 6-12 months.