Biologic Background
Common idea: Lymph is ~90% reabsorbed in venous end
New theory: NO reabsorption in capillary!
RT decreases no. of dermal…
RT -> hypoxia -> lymphatic endothelial senescence -> increased lymphangiogenesis (which is abnormal, with increased permeability)
Factors
Head and Neck Cancer
Breast Cancer
Gynecologic Cancer
Assessment
Circumference measure
- Conventionally… Elbow, 10cm proximal and distal, wrist, MCP
- Difference ≥2cm
Perometer
- Utilizes an array of moving optoelectronic infrared sensors
- No reimbursement.. Only 3 institutions
Bioimpedence
- Limb index ratio = resistance of unaffected/affected
- >1.139 if the affected arm was the dominant arm
- >0. …
Radionuclide lymphoscintigraphy
- Uptake pattern of regional LNs.
- Uptake pattern of main lymphatic vessels
- Presence of dermal backflow
- Presence of collateral lymphatic vessels
Indocyanine green (ICG) lymphography
Ultrasound
- Skin and SQ thickness..
CT lymphangiography
- Pts prefer over MR bc it’s quick and cheap (1/10).
MR lymphangiography
- T2 high SI. Contrast-enhancement is required
Treatments
Intensive Care
- Skin care
- Exercise/movement
- MLD
- MLB (multi-layer bandage)
- ±IPC
Maintenance
Bandages and Compression
MLB
Tubular bandage -> elastic fixation bandage -> padding (for even-pressurizing) -> short-stretch (저탄력) bandage
Pneumatic compression
More chambers than DVT prophylactic compressor
Elastic stocking
Arms: class 1-2
Legs: class 3-4
Differences between stockings & bandages
- Working pressure increase is more evident in bandage
Alternative compression materials
- Adjustable compression wraps, with foam block,
Pharmacologic treatment
- Flavonoids:entelon
- Naftazone?
- On clinical trial
- Tacrolimus?
Surgical Treatment
Lymphovenous anastomosis (LVA)
Vascularized LN transfer (VLNT)
Liposuction
AMC pf 권진근
Lower level LASER Therapy (LLLT)
(LITT, 1st gen)
(PDT, 2nd gen)
(PBM, 3rd gen)
- Reimbursement: up to 20 min, >2 min for each location
Physical grounds
| Continuous LASER | Pulsed LASER | |
| DNA impairement | Activates repair mechanism | |
Surgical Methods
AMC pf 권진근
Past: Charles’ procedure
Current: Microsurgery
Lymphatico-venous anastomosis; LVA, 림프관정맥간 문합술
Making detour to Vein
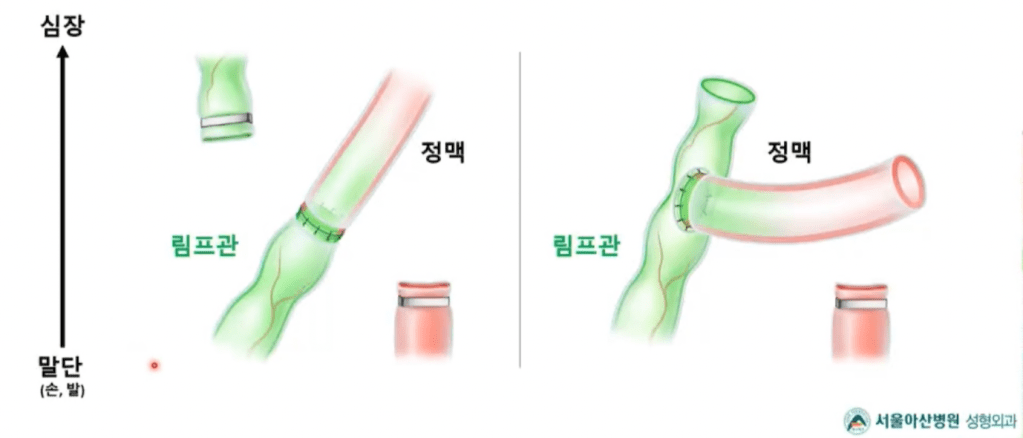

- Preop evalulation
- MRI / ICG lymphangiography / USG
- vein should be in proximity, functioning lymphatic duct is essential
- Intraop evaluation
- Milking test
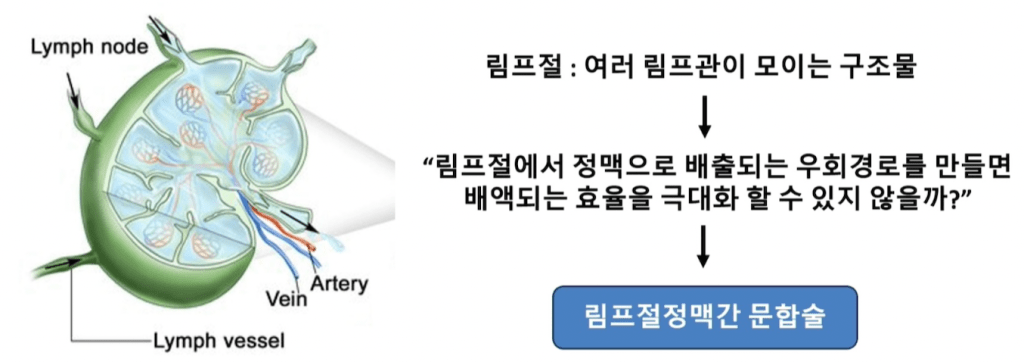
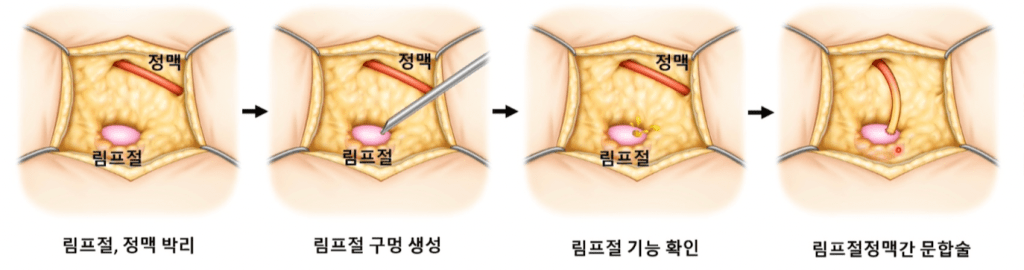
Lymph node to vein anastomosis; LNVA 림프절정맥간 문합술
Vascularized lymph node transfer; VLNT 혈관문합 림프절 이식수술
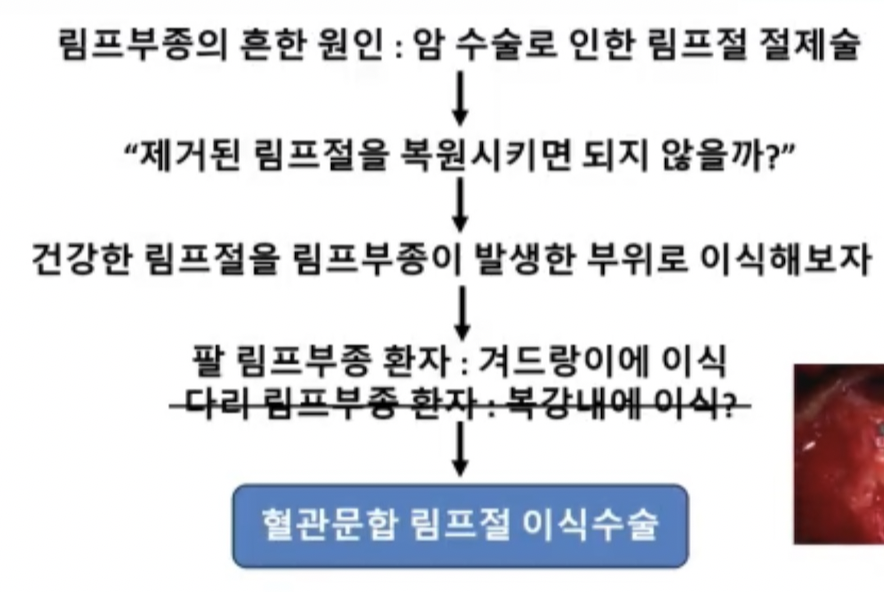

Omental VLNT
Inguinal VLNT
Indication
- Already had LVA, having contraction
Removing adipose tissue
- Ablative surgery
- Liposuction
- Usually 1L, up to 5L
Biobridge insertion
FDA-approved
No 5yr f/u data.
Postop management
Can walk on the day of the surgery!
Compression bandage
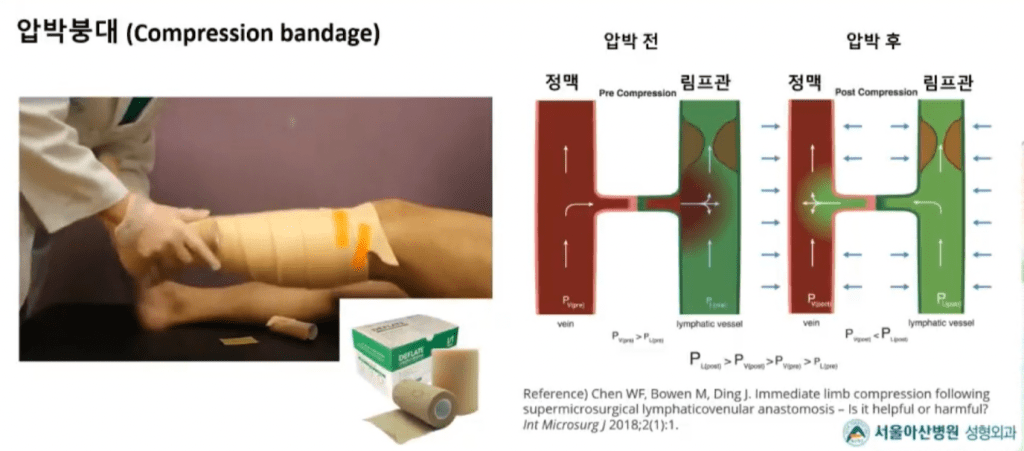
- 24hr for 6 months, and then tapering
Weight reduction, hydration
Lymphatic Duct Injuries
Traumatic thoracic duct cyst
Surgical management
- Mass removal + TD mass ligation
- Complete excision 이 표준
- 흉관 mass ligation이 동반
Intervention
Observation
Nontraumatic chylothorax leak
Due to e.g., lymphoma..
Duct ligation – not essential
- Hard to find a leak point
- Chemical pleurodesis – may be curative
- Chemotherapy – may regress with disease
- Radiotherapy – should pinpoint the leakage site. Highly effective, but localization is always the problem.