2025.03.12 서원영
human의 LD50/60는 얼마일까? 3.5Gy-7GY사이 어딘가에 있을 것..
1. Acute radiation syndrome (ARS)
– Human data; from RT, Hiroshima & Nagasaki, Marshallese, Chernobyl, Tokaimura
; To date, worldwide, about 400 humans have suffered from ARS
2. Early lethal effects
– Early radiation lethality : within a few weeks, specific high-intensity exposure
– ‘Prodromal syndrome‘: early Sx appeared, last for a limited period
à clear-up for a few days à latent period à development of life-threatening syndrome (Fig 8.1)
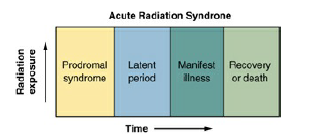
Figure 8.1 Illustrating the stages of the acute radiation syndrome. Following total body irradiation, the prodromal syndrome develops—the intensity and length depending on the dose. There follows a latent period when symptoms disappear, followed by the development
– Mode of death ß magnitude of the dose
① (high dose level) Cerebrovascular syndrome: 100Gy, death in 24-48 hrs, from neurologic and cardiovascular breakdown
② (intermediate dose level) Gastrointestinal syndrome: 5-12 Gy, death in 9-10 days, extensive bloody diarrhea and destruction of the GI mucosa
③ (lower dose level) Bone-marrow death or hematopoietic syndrome: 2.5-5 Gy, death in weeks-2months, effects on the blood-forming organs
3. The Prodromal radiation syndrome
– Symptoms vary with respect to time of onset, maximum severity, duration, size of the dose
– Tens of gray à all phases of the syndrome within 5-15 mins, maximum reaction reached by about 30 mins, persist for a few days
– Severe prodromal syndrome à poor Px
- Signs and symptoms of human prodromal syndrome → Two main groups
① GI: anorexia, nausea, vomiting, diarrhea, intestinal cramps, salivation, fluid loss, dehydration, weight loss
② Neuromuscular: easy fatigability, apathy or listlessness, sweating, fever, headache, hypotension
(Table 8.1) Symptoms of the Prodromal Syndrome
| Neuromuscular | Gastrointestinal |
| Signs and Symptoms to be Expected at about 50% Lethal Dose | |
| Easy fatigability | Anorexia |
| – | Nausea |
| – | Vomiting |
| Additional Signs to be Expected After Supralethal Doses | |
| Fever | Immediate diarrhea |
| Hypotension | |
- At doses that would be fatal to 50% of the population à anorexia, N/V, easy fatigability
- Duration of latent period: inversely proportional to the dose
eg. Progressive worsening from prodromal signs and symptoms directly into the manifest illness phase: an indicator that the dose was very high
– Diagnosis of ARS by ‘fall of absolute lymphocyte count’ after an exposure as low as 0.5 Gy: best & most useful lab test to determine the level of radiation exposure in the early phase of observation
: circulating lymphocytes, the most radiosensitive cell line
– ‘chromosomal aberration analysis from cultured circulating lymphocytes‘
– lower limit of detection of a dose by using the cytogenetic method : 0.2 Gy of r-rays or x-rays
4. The Cerebrovascular syndrome
– 100 Gy total body dose of r– rays à death in 24-48 hrs
: all organ systems are seriously damaged
(cerebrovascular damage brings death very quickly)
- ‘death occurs before other symptoms have time to appear’
– severe N/V(mins) à disorientation, loss of coordination of muscular movement, respiratory distress, diarrhea, convulsive seizure, coma à death
<case 1>
– 1964, M/38, working in uranium-235 recovery plant, accidental nuclear excursion
– total body dose of 88 Gy (22 Gy of neutrons, 66 Gy of r-rays)
– Immediate: abdominal cramps, headache, vomiting, incontinent bloody stool
– next day: comfortable but restless
– 2nd day: fatigued, apprehensive, short of breath, impaired vision, difficulty in maintenance of BP
– died in 49 hrs
<case 2>
– 1958, Nuclear criticality accident at Los Alamos
– total body dose of 39-49 Gy (max. 120 Gy)
– a state of shock immediately: unconscious within a few mins à no lymphocytes in 8 hrs, urinary shutdown
– died in 35 hrs
à exact & immediate cause of death are not fully understood
à usually attributed to events taking place within the central nervous system, but much higher doses are required to produce death if the head alone is irradiated rather than the entire body
à damage to microvasculature à an increase in the fluid content of brain (d/t leakage from small vessels) à buildup of pressure within the bony confines of the skull
5. The Gastrointestinal syndrome
– > 10 Gy total body dose à GI Sx. à death in 3-10 days
– N/V, prolonged diarrhea, loss of appetite, sluggish & lethargic
* prolonged diarrhea: > 10 Gy à inevitably fatal
- signs of dehydration, loss of weight, emaciation, complete exhaustion à death
– depopulation of epithelial lining of GI tract

Figure 8.3 The gastrointestinal epithelium is an example of a classic selfrenewal tissue. Stem cells in the crypts divide rapidly and provide cells that differentiate to form the lining of the villi. A single cell layer separates the blood supply within the villus from the contents of the gastrointestinal (GI) tract. An exposure to radiation kills cells in the crypts, cutting off a supply of cells to cover the villi. As a consequence, the villi shrink and, eventually, the barrier between blood supply and the contents of the GI tract is compromised, leading to a loss of fluids and massive infections.
– 10 Gy à sterilize a large proportion of the dividing cells in the crypt
(not to differentiated & functioning cells)
à villi shorten & shrink in a few days à completely denuded
– rate & time vary by the dose, species (human: after 10 days)
<case 1>
– 1946, M/32
– total body dose of 11-20 Gy (hands: 300 Gy)
– vomiting in hrs, 6th day paralytic ileus à 7th day, liquid stools with occult blood à 9th day, circulatory collapse, jaundice, spontaneous hemorrhage à died
– at autopsy showed ‘small intestine change’: mucosal surface edematous & erythematous, membranous exudate microscopically, complete erosion of epithelium, denuded surface with bacteria (E.coli)
<case 2>
– Chernobyl, firefighters
– died within 7-10 days including bone marrow transplants
– symptoms characteristics of GI syndrome
6. The Hematopoietic syndrome
– 2.5-5 Gy à damage to the hematopoietic system
– mitotically active precursor cells are sterilized à RBC, WBC, plt diminished
– delayed for some weeks for cell count reaches minimum value
– ‘LD50‘: 50% lethal dose à def) the dose of any agent or material that causes a mortality rate of 50% in an experimental group within a specified period
<Fig 8.4> Mortality rate of rhesus monkeys at 30 days after a single total body exposure to x-rays

- upto a dose exceeding 2 Gy, no animals die
- about 8 Gy: kills all the animals exposed
- between the two doses: very rapid increase in the percentage of animals killed as the dose increases
- LD50 of 5.3 Gy
– human: much more slowly than other mammals, peak incidence of death d/t hematopoietic damage at 30 days after exposure à continues upto 60 days à LD50 in human expressed as LD50/60
– dose of LD50 à prodromal syndrome (chief symptoms of N/V) à latent period (symptom-free interval) à after 3 wks, chills, fatigue, petechial hemorrhage, oral ulceration, hair loss à infection, fever, bleeding, anemia from bleeding d/t low plt (not by RBC depression) à death

- Attempts to estimate the LD50/60
– Hiroshima & Nagasaki: 3.5 Gy for young healthy adults without medical intervention
à a number of instances in which young men and women have received total body irradiation up to a dose of around 4 Gy and recovered under conservative care
- Chernobyl: closer to 7 Gy – antiobiotics were available
– ‘rescue dose‘ required in BMT
: the number of transplanted BM cells required to recover from a supralethal dose
– negative correlation between body weight & hematopoietic stem-cell concentration
7. Pulmonary syndrome
– Survivors of hematopoietic syndrome with exposure of 8Gy or more developed inflammatory pneumonitis.
<Fig 8.6>

Figure 8.6 Illustrating how the pulmonary syndrome appeared in a few individuals exposed to a total body dose of 8 to 10 Gy but who survived the hematopoietic syndrome by intensive treatment with antibiotics, transfusions, and hematopoietic growth factors (HGFs). They died much later, about 130 days after irradiation, with inflammatory pneumonitis. G.I., gastrointestinal; LD50, 50% lethal dose.
8. Cutaneous radiation injury
- apparent within hours or may not be seen for weeks
- itching and tingling to epilation, erythema, edema, progressing to dry desquamation, wet desquamation, ulceration, and necrosis
- epilation: about 3 Sv, erythema: about 6 Sv
à with increasing dose of > 10Sv: injury worsens progressively
9. Symptoms associated with the acute radiation syndrome
- Diagnosis and Treatment of Radiation Injuries
<Table 8.3> – prodromal syndrome in the period soon after irradiation

<Table 8.4> – later critical phase

– 1-2 Gy à little effect, > 8 Gy à 100% lethality
- nature of symptoms, severity, time of onset: useful predictor of eventual outcome
ex) severe immediate diarrhea: supralethal dose à any treatment is likely to be ineffective à useless
10. Treatment of radiation accident victims exposed to doses close to the LD50/60
1) < 4-5 Gy – watch carefully
– Tx: antibiotics, fresh plt (no prophylactic transfusion)
2) > 5 Gy – death from hematopoietic syndrome in 3-4 wks is possibile
– avoid infection, bleeding, physical trauma
– ‘use of BMT’
: for 4 Yugoslav scientists – initially estimated as 7 Gy
à All grafts rejected, but the exposed individuals survived anyway à later estimation: 4 Gy
* dose of LD50 or higher à peripheral lymphocytes disappear before 24 hrs
: estimate total body dose by counting chromosome aberrations in stimulated lymphocytes
à not possible
– window of dose within BMT useful à very small: 8-10 Gy
11. Triage
- immediate need is to know what doses are involved à however, not monitored in general
1) The average time to emesis decreases with increasing dose.
- individual responses variable à only rough guidance
- < 1 Gy: few individuals vomit, >2 Gy: most vomit
<Fig 8.8>

2) The decline in the lymphocyte count allows an estimate to be made of the total body radiation exposure.
<Fig 8.9>

3) (With a cytogenetic laboratory available) The best method is to measure the incidence of chromosomal aberrations in peripheral lymphocytes stimulated to divide in vitro.
– high doses à lymphocytes disappear quickly (several limitations)
12. Survivors of serious radiation accidents in the United States
– for 50 yrs, 70 workers from 13 accidents
– shorten lifespan, early malignancies after a short latent period, rapidly progressing lenticular opacities à not observed
13. Radiation emergency assistance center
– Medical Sciences Division of the Oak Ridge Institute for Science and Education
: Radiation Emegency Assistance Center/Traning Site (REAC/TS)