THE INTRODUCTION OF FRACTIONATION
Radiobiologic experiments, France (1920s~1930s) – sterilization of rams
- A single dose of radiation: extensive skin damage to the scrotum
- Fractionation of the radiation: sterilization w/o producing unacceptable skin damage
-> Fractionation of the radiation dose produces better tumor control for a given level of normal tissue toxicity than a single large dose.
THE FOUR Rs OF RADIOBIOLOGY
Four Rs of radiobiology: the efficacy of fractionation
- Repair of sublethal damage
- Reassortment of cells within the cell cycle
- Repopulation
- Reoxygenation
1,3 – spares normal tissues
2,4 – ↑ damage to the tumor
The advantages of prolongation of treatment
- To spare early reactions
- To allow adequate reoxygenation in tumors
Cf. Excessive prolongation allows surviving tumor cells to proliferate during treatment.
THE STRANDQUIST PLOT AND THE ELLIS NOMINAL STANDARD DOSE SYSTEM
1 – Strandquist plot
- the slope of the isoeffect curve for skin ≈ 0.33
- Total dose for an isoeffect ∝ T0.33

2 – NSD (nominal standard dose) system by Ellis: separating the effects of T and N
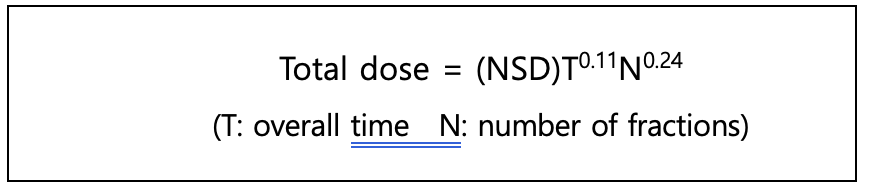
This system is based on skin-reaction data =>It does not predict late effects
Time – a single power function => not accurate.
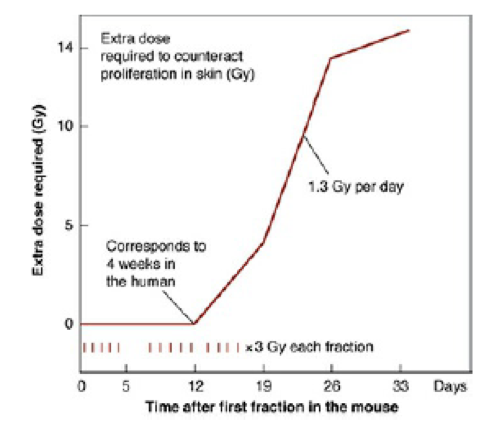
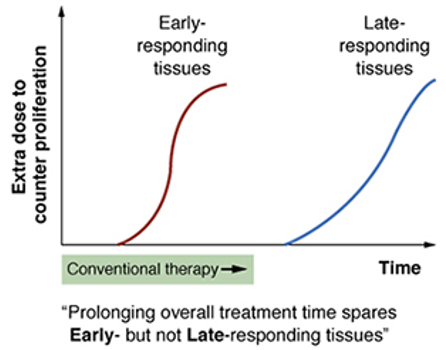
PROLIFERATION AS A FACTOR IN NORMAL TISSUES
1 – The extra dose required to counter proliferation: sigmoidal curve
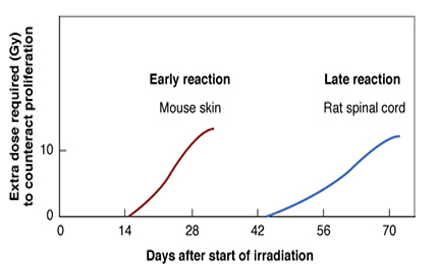
2 – Early vs late responding tissues
- Early responding tissues: skin, mucosa, intestinal epithelium.
Late responding tissues: spinal cord, kidney, lung.. - Extra dose required to counteract proliferation (produce a given level of damage for a fractionated protracted regimen) is different.
The delays are much longer in humans. - Prolonging overall time within the normal radiotherapy range has little sparing effect on late reactions but a large sparing effect on early reactions. (∵ 6 or 8 weeks is never long enough to allow the triggering of proliferation in late responding tissues)
THE SHAPE OF THE DOSE-RESPONSE RELATIONSHIP FOR EARLY- AND LATE-RESPONDING TISSUES
Response to changing fractionation
- fewer and larger dose fractions more severe late reaction
=> d/t differences in repair capacity / shoulder shape of the dose-response curves - α/β ratio is the dose at which cell killing by linear (α) and quadrantic (β) components are equal (αD=βD2, D= α/β)
- early effects – larger α/β ≈10 Gy
- late effects – small α/β ≈2 Gy

Dose-response curves for organ function (≈ tolerance of normal tissue)
- Organ function must be distinguished from those for clonogenic cell survival
the proportion of functional cells >> the proportion of clonogenic cells
: more curved, larger shoulder : straight, small shoulder
Evidence for the difference of the dose-response relationship for early and late
- 임상에서, many small dose에서 a few large fraction으로 변경할 때, 동일한 early effect가 나타나게 titration해도 a few large fractions more severe late effects
- Clinical trials of hyperfractionation (bid for 6-7 wks)
: greatly reduced late effects with equal early effects and tumor control
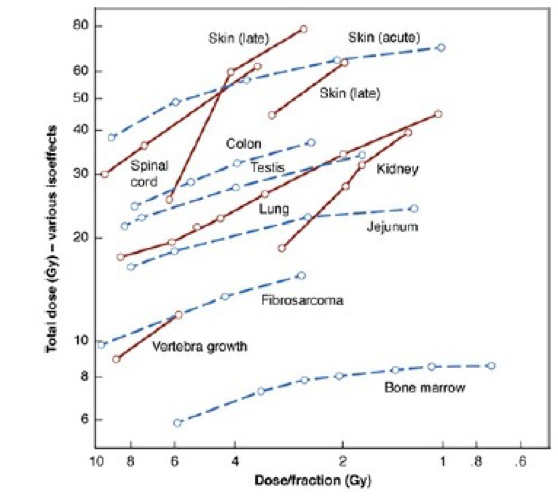
=> Late effect tissues are more sensitive to changes in fractionation patterns than early responding tissues - Experiments with laboratory animals (Fig 23.7)
: the isoeffect curves are steeper for a range of late effects
Ex) Early: skin, jejunum, Late: lung, spinal cord
POSSIBLE EXPLANATIONS FOR THE DIFFERENCE IN SHAPE OF DOSE-RESPONSE RELATIONSHIPS FOR EARLY- AND LATE-RESPONDING TISSUES
Radioresistance and cell cycle
- late S phase – most resistant
- early G1(≈G0 phase, resting cell) – second resistant phase, slowly growing cells
Two quite different radioresistant cell population
- oliferating so fast : S phase is major portion of the cycle
- acute-responding normal tissues, tumor
- redistribution of the cell cycle (= “self-sensitizing” activity)
- proliferating so slowly : many cells are in early G1, G0
- late-responding normal tissues
- resistance with small doses/fx 이었다가 disappears at larger doses/fx
FRACTION SIZE AND OVERALL TREATMENT TIME
INFLUENCE ON EARLY- AND LATE-RESPONDING TISSUES (1980년대까지 몰랐음)
| Fraction size | Overall Tx time | |
| Late responding tissues | Dominant factor | Little influence |
| Acute responding tissues | Both determine the response | |
ACCELERATED REPOPULATION
1 – Accelerated repopulation
The triggering of surviving cells (clonogens) to divide more rapidly as a tumor shrinks after irradiation or treatment with any cytotoxic agent.

2 – Accelerated repopulation in human tumors – radiotherapy for head and neck cancer
- Accelerated repopulation starts about 28 days after initiation of RT.
- About 0.6 Gy/day is needed to compensate for this repopulation.
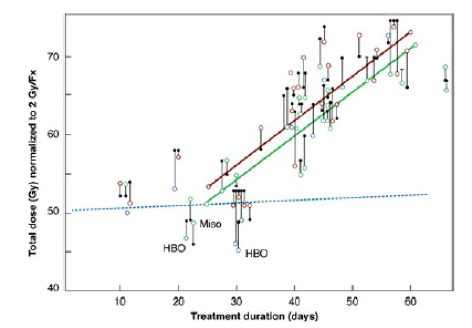
=> It may be better to delay the start than to introduce interruptions during Tx.
Too long overall treatment time the effectiveness of later dose fractions ↓
THE IMPORTANCE OF OVERALL TREATMENT TIME
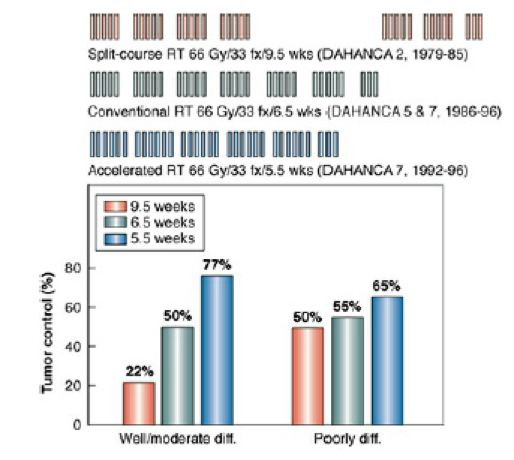
- Local control is lost if overall treatment time is prolonged.
- H&N cancer : 1.4% local control per each day prolonged
- Cervix carcinoma: 0.5% local control per each day prolonged
MULTIPLE FRACTIONS PER DAY
Prolongation of Tx
- Advantages of prolongation of treatment
- spare early reactions
- allow adequate reoxygenation in tumors
- Disadvantages of excessive prolongation of treatment
- late injury를 sparing하지않으면서, acute reaction을 감소시키는 것으로 현혹시킬 수 있다.
- allow the surviving tumor cells to proliferate during treatment
Hyperfractionation
basic aim: to further separate early and late effects
=> ↓ late effect, ↔ or ↑ tumor control, ↔ or sl. ↑ early effect
EORTC 22791 of head-and-neck cancer (T2-3, N0-1, OPx less than 3cm)
- 80.5 Gy/70 fx (1.15 Gy twice per day), 7weeks vs 70 Gy/35 fx, 7weeks
- 5YR local tumor control ↑ (40 59%, p=0.02) : improved survival trend (p=0.08)
- No increase in late complications
- Unequivocal advantage for hyperfractionation in oropharyngeal ca
Accelerated treatment
The intent
- ↓ repopulation in rapidly proliferating tumors
- => ↔ late effect, ↑ tumor control, ↑ early effect
EORTC 22851 trial of head-and-neck cancer T2-4 except hypopharynx
- 72 Gy/45 fx (1.6 Gy, 3fx/day), 5weeks with rest of 2 weeks in the middle
vs 70 Gy/35 fx, 7weeks - Locoregional control ↑ 15% (p=0.02)
- No survival advantage, DSS은 p=0.06으로 AF를 선호하는 경향
- Increased acute effects (expected)
- Unexpected increase in late effects including lethal complication
CHART (Continuous hyperfractionated accelerated radiation therapy)
Aim
- short Tx time ↓ tumor proliferation
- low dose per fraction minimize late effects
Result
- 50.4-54Gy/36fx over 12 consecutive days,
- 1.4-1.5 Gy/fx, 3fx/day with 6 hr interval
- Local tumor control is good because overall Tx time is short
- Most late effects are acceptable because the dose per fraction is small
- An exception is the spinal cord
- : several myelophathies occurred at 50 Gy because the time between fractions (6 hrs) was too short
HYPOFRACTIONATION: RENEWED INTEREST
1970~1980: Increasing number of fraction was a trend.
Recent interest
- α/β is low in some tumors: ex) prostate cancer
- RS and SBRT
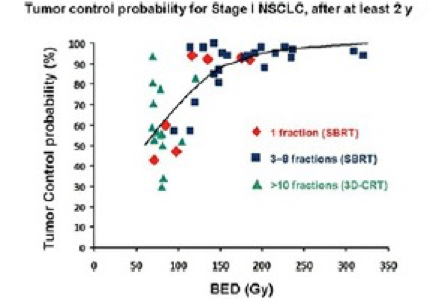
- Carbon ion therapy: small number of large dose fractions
- Not clear whether the success is caused by superior dose distribution or relatively high LET.
USING THE LINEAR-QUADRATIC CONCEPT TO CALCULATE EFFECTIVE DOSES IN RADIOTHERAPY
Biologic effect of a single acute dose
E = αD + βD2
(E : biologic effect D : single acute dose)
Biologic effect of fractionated dose
E = n(αd + βd2)
= (nd)(α + βd)
= = (α)(nd)(1+ d/ (α/β) )
(n : no of fraction d: dose/fx)
- α/β choice : late-responding tissue 3 Gy, early-responding tissue 10 Gy
late responding tissue와 별 차이가 없는 암종: breast, prostate ca.
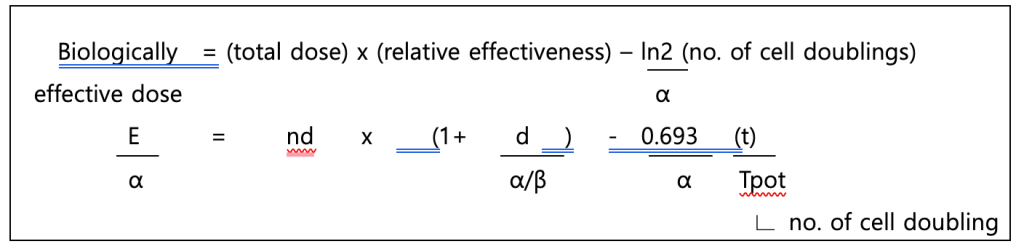
Allowance for tumor proliferation
N = N0eλt (N: number of clonogens at time t, N0 : initial number of clonogens)
λ= ln2 /Tpot = 0.693 /Tpot (Tpot : potential doubling time of the tumor, by Fowler)
The decrease in the number of clonogens because of cell killing by the fractionated radiation regimen is balanced to some extent by cell division of the surviving clonogens.
The biologic effect in equation (2) now becomes
E = n(αd + βd2) – 0.693 t / Tpot