The origins of radiation protection
- Early recognition of radiation hazards led to British recommendations in 1915.
- Second International Congress of Radiology (1928) established international X-Ray and Radium Protection Committee which was remodeled into two commissions after WWII; ICRP (The International Commission on Radiological Protection) and ICRU (The International Commission on Radiation Units and Measurements)
- In the US, the Advisory Committee on X-Ray and Radium Protection was set up in 1928, and renamed as NCRP (The National Council on Radiation Protection and Measurements) in 1946
Organizations
- Data Analysis/Risk Estimation: considered “scholarly” committees, less compelled to make recommendations without adequate data
- United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR): International body since 1958, latest report in 2013.
- Biological Effects of Ionizing Radiation (BEIR) Committee: US committee, first report in 1956 known as BEAR(Biological Effects of Atomic Radiation), latest BEIR VII in 2006.
- The committees that formulate the concepts for use in radiation protection and recommend maximum permissible levels
- ICRP and ICRU: International body, restructured in 1950, often leads in concepts and limits; has no jurisdiction over anyone and can do no more than recommend
- NCRP: US body chartered by Congress; often follows ICRP but has differences; neither body has any jurisdiction to enforce their recommendations
- US Regulatory Agencies
- Environmental Protection Agency (EPA): Provides guidance to federal agencies (e.g., sets radon action levels).
- Nuclear Regulatory Commission (NRC): Controls use of reactor by-product materials in states with agreement
- Occupational Safety and Health Administration (OSHA): Regulates in non-agreement states.
- Department of Energy (DOE): Responsible for radiation safety regulations at all of its facilities operated by contractors
Quantities and units
- Dose = Absorbed Dose (D): Energy absorbed per unit mass. SI unit: Gray (Gy = J/kg). Old unit: rad (1 Gy = 100 rad).
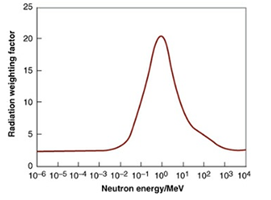
- Radiation Weighting Factor (WR): Dimensionless multiplier used in radiologic protection to place biologic effects (risks) from exposure to different types of radiation on a common scale. It is chosen by ICRP as representative of relative biologic effectiveness (RBE), applicable to low doses and low dose rates.
| Radiation type | Radiation weighting factors |
| Photons | 1 |
| Electrons and muons | 1 |
| Protons and charged pions | 2 |
| α-particles, fission fragments, heavy ions | 20 |
| Neutrons | A continuous curve as a function of neutron energy (Figure 16.2) |
- Equivalent Dose: Absorbed dose averaged over tissue/organ x WR. Unit: Sievert (Sv). (ICRP recommended the new name, Radiation Weighted Dose). For mixed radiation fields, sum the individual weighted doses.
- Effective dose: Risk of stochastic effects of nonuniform radiation as if the whole body had received a uniform exposure. Different tissues have different sensitivity to stochastic effects.
- Tissue Weighting Factor (WT): Represents relative contribution of each tissue/organ to total detriment from uniform whole-body irradiation, reflecting differing sensitivities. Values given in Table 16.2.
- Effective dose = Σ absorbed dose X WR X WT
| Organ/Tissue | Number of tissues | WT | Total contribution |
| Lung, stomach, colon, BM, breast, and remainder | 6 | 0.12 | 0.72 |
| Gonads | 1 | 0.08 | 0.08 |
| Thyroid, esophagus, bladder, and liver | 4 | 0.04 | 0.16 |
| Bone surface, skin, brain, and salivary glands | 4 | 0.01 | 0.04 |
- Committed Equivalent Dose 예탁등가선량: Equivalent dose integrated over 50 years after intake of a radionuclide. For radionuclides with effective half-lives of up to 3 months, the committed equivalent dose is equal to the annual equivalent dose in the year of intake. If longer half-life, higher committed equivalent dose.
- Committed Effective Dose 예탁유효선량: Sum of committed equivalent doses x WT.
- Collective Equivalent Dose 집단등가선량: Average equivalent dose to a population X number of persons exposed (Unit: person-sievert)
- Collective Effective Dose 집단유효선량: Average effective dose to a population X number of persons exposed (Unit: person-sievert
- Collective Committed Effective Dose 집단예탁유효선량: In the case of a population ingesting or inhaling radionuclides that deposit their dose over a prolonged period – the integral of the effective dose over the entire population out to a period of 50 years.
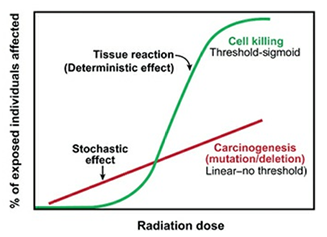
Tissue Reactions (formerly Deterministic Effects):
- Result from cells being killed and removed from an organ or tissue.
- Have a dose threshold below which effects aren’t seen.
- Severity increases with dose above threshold.
- Dose-response curve: Threshold-sigmoid (Figure 16.3).
- Examples: Effects on fertility, lethality from total body exposure, organ failure.
Stochastic Effects:
- Result from cells that are not killed but mutated
- All-or-nothing effect; severity is independent of dose, but the probability of occurrence increases with dose.
- Conservative to assume no dose threshold for protection purposes.Dose-response curve: Linear or linear-quadratic, no threshold (Figure 16.3).
- Examples: Cancer, heritable effects,
Principles of radiation protection
- Framework of NCRP 1993 recommendations
- Justification: justify radiation exposure based on expected benefit.
- Patients: the diagnostic or therapeutic benefit should outweigh the risk.
- Occupational: the radiation risk must be added to and compared with other risks in the workplace.
- Research: In cases in which the individual receives no benefit, the benefit to society must outweigh the risks.
- ALARA: Keep exposures As Low As Reasonably Achievable.
- Limitation: Apply individual dose limits.
- Justification: justify radiation exposure based on expected benefit.
- Objectives:
- To prevent clinically significant radiation-induced tissue reactions (stay below thresholds).
- To limit the risk of stochastic effects to a reasonable level.
Basis for exposure limits
- Evolved from “tolerance dose” (1930s, considering acute effects such as erythema) to “maximum permissible dose” (1950s, considering late effects such as cancer).
- By 1980s, comparing risk estimates for deleterious effects of radiation with accidental mortality rates in safe industries.
| End point | Risk estimate |
| Severe mental retardation in exposure of embryo/fetus (8-15wk) | 40%/Sv |
| Carcinogenesis in general population (low dose, low dose rate) | 5%/Sv |
| Heritable effects in general population | 0.2%/Sv |
| NCRP | ICRP | |||
| Occupational exposure | ||||
| Stochastic effects: effective dose limits | ||||
| Cumulative | 10 mSv x age | 20 mSv/y averaged over 5y | ||
| Annual | 50 mSv/y | 50 mSv/y | ||
| Tissue reactions: dose equivalent limits for tissues and organs (annual) | ||||
| Lens of eye | 50 mSv/y | 20 mSv/y averaged over 5y Not more than 50 mSv in any year | ||
| Skin, hands, and feet | 500 mSv/y | 500 mSv/y | ||
| Embryo/fetus exposure | ||||
| Effective dose limit after pregnancy declared | 0.5 mSv/mo | Total of 1 mSv to embryo/fetus | ||
| Public exposure (annual) | ||||
| Effective dose limit, continuous or frequent exposure | 1 mSv/y | 1 mSv/y (No distinction between frequent and infrequent) | ||
| Effective dose limit, infrequent exposure | 5 mSv/y | 1 mSv/y | ||
| Dose equivalent limits; lens of the eye | 15 mSv/y | 15 mSv/y | ||
| Skin and extremities | 50 mSv/y | 50 mSv/y | ||
| Education and training exposure (annual) | ||||
| Effective dose limit | 1 mSv/y | No statement | ||
| Dose equivalent limit for lens of eye | 15 mSv/y | No statement | ||
| Skin and extremities | 50 mSv/y | No statement | ||
| Negligible individual dose (annual) | 0.01 mSv/y | No statement | ||
Limits for occupational exposure (NCRP)
- Not include natural background radiation or radiation for medical purposes
- Stochastic Effects (Effective Dose):
- No occupational exposure should be permitted until the age of 18 years.
- The effective dose in any year should not exceed 50 mSv
- The individual worker`s lifetime effective dose should not exceed age in years x 10 mSv
- ICRP: cumulative 20mSv/y averaged over 5y
- If individual work with maximum dose permitted from age 18 to 65, NCRP total 650 mSv, ICRP total 940 mSv, NCRP allows more radiation in earlier ages, ICRP allows mor radiation in later ages.
- Stochastic Effects (Effective Dose):
- Tissue Reactions (Equivalent Dose – Annual):
- Lens of the eye: 50mGy per year (an appropriate RBE should be used if radiation other than x-rays is involved.
- Localized area of skin, hands, feet: 500 mSv per year
As low as reasonably achievable
- The dose limits referred to previously are all subject to the concept of ALARA
- the ultimate problem is determining what is “reasonable.”
- ALARA has a cash value of about $1,000 per 10 mSv. (Low dose)
- the cash value of avoiding a 10-mSv exposure may be closer to $10,000. (High dose level when lifetime dose limit is threatened)
Protection of embryo/fetus
- No recommendation until pregnancy is declared.
- NCRP: 0.5 mSv/month to embryo/fetus.
- ICRP: 2 mSv to the surface of woman’s abdomen for remainder of pregnancy.
- Special care needed for internally deposited radionuclides.
Emergency occupational exposure
- Only actions involving the saving of life justify acute exposure more than the annual effective dose limit.
- Use volunteers, preferably older workers with low lifetime dose.
- For actions not saving life, control exposure at occupational limits if possible; if not, limit to 0.5 Sv (NCRP/ICRP recommendation).
- In lifesaving or equivalent purposes, workers exceeding 0.5 Sv must understand risks of acute effects and cancer.
Exposure of persons younger than 18 years of age
- NCRP: For educational and training purposes, annual effective dose limit 1 mSv.
Exposure of members of the public (nonoccupational limits)
- Risk of accidents and death for members of public: 10-4 to 10-6 per year.
- Everyone is exposed to natural background radiation of about 1 mSv annually, excluding radon, which may result in a mortality risk of 10-4 to 10-5 annually.
- NCRP recommendation: Medical exposures are excluded
- Continuous/Frequent exposure: Annual effective dose limit 1 mSv.
- Infrequent exposure: Annual effective dose limit 5 mSv.
- Tissue Reactions: Lens 15 mSv, Localized area of skin, hands, feet 50 mSv.
Exposure to indoor radon
- Levels vary greatly by locality. Concentrations increased by insulation.
- Solid progeny sticks to particles of dust and moisture and is deposited on bronchial epithelium causes local irradiation.
- Air concentration of 20 Bq/m3 = effective dose to the bronchial epithelium of 1 mSv per year.
- Average home radon concentration 20-60 Bq/m3
- Action level by EPA 148 Bq/m3 -> Remedial action should be taken.
- BEIR VI: about 1 in 10 to 1 in 7 of all lung cancer deaths can be attributed to radon. Perhaps one-third could be avoided by reducing radon in homes with radon above the action level.
De minimis dose and negligible individual dose
- Concept: Dose below which further efforts to reduce radiation are unwarranted.
- (legal responsibilities on NCR)
- NCRP considers Negligible individual dose as 0.01 mSv/year.
- This dose is associated with a risk of death between 10-6 and 10-7 considered trivial compared to risks of fatality with ordinary activities.
Radiation detriment
- Concept introduced by ICRP to quantify the harmful effects of radiation exposure to different parts of the body taking into account the severity of the disease in terms of lethality, loss of QOL, years of life lost).
- 5.5%/Sv for cancer, 0.2%/Sv for hereditary effect → total 5.7%/Sv
- Average annual dose of radiation worker (~2 mSv/yr) leads to detriment (~1 in 10,000) comparable to death rate in “safe” industries.
The history of the current dose limits
- 1956 limit (5 R/yr or 50 mSv/yr) based on fruit fly genetics
- Concern shifted from heritable effects to carcinogenesis over time.
- ICRP (1991) added 20 mSv/yr average limit; NCRP (1993) added Age x 10 mSv cumulative limit to address increased cancer risk perception.
- Both aimed for risks comparable to “safe” industries (~3% cancer mortality risk).
- ICRP and NCRP only make recommendations. US NRC has legal responsibility and limits annual dose to 50 mSv but has not adopted cumulative limit.
- Table 16.6 Cancer risks for a radiation worker receiving the maximum permissible dose from age 18 to 65 years
| Rule | Total dose | Cancer incidence | Cancer mortality |
| NRC 50mSv/y | 2.35 Sv | 19.0% | 10.8% |
| NCRP 10mSv x age | 0.65 Sv | 6.1% | 3.3% |