Cataracts of the ocular lens
- A cataract is an opacity in the normally transparent lens.
- Among three major forms of cataracts (Cortical, Nuclear, Posterior subcapsular), posterior subcapsular (psc) cataracts are most closely associated with ionizing radiation.
- Lens anatomy Figure 13.1

- Throughout life, a small population of epithelial cells just anterior of the lens equator divide and differentiate into lens fiber cells, which make up the majority of the lens mass.
- Radiation damage to the dividing/differentiating epithelial cells is thought to initiate cataracts. Damaged cells migrate to the posterior pole, accumulate, and cause opacity.
Lens opacification in experimental animals
- Mice are very sensitive; low doses (1mGy of fast neutron or few tens of mGy of x-rays) produce changes.
- Radiation seems to shorten the latent period to cataract.
- Neutrons and densely ionizing radiations are very effective (high RBE) at inducing cataracts. RBE for neutrons increases significantly at low doses (can reach 50 or more) compared to high doses (around 10).
Radiation cataracts in humans
- Stimulated interest after cataracts were observed in cyclotron workers and A-bomb survivors after WWII.
- Radiation cataractogenesis
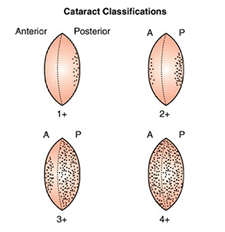
- 1. small posterior dots/vacuoles, possibly a central opacity at the posterior pole
- 2. dots and vacuoles coalesce
- 3. granular opacities and vacuoles appear in the anterior subcapsular region
- Absence of this sequence exclude radiation as a cause.
- Location at posterior visual axis can disproportionately affect vision even with small size and may require surgery to restore vision.
- Merriam and Focht classification system (stages 1-4) describes severity. Figure 13.3
- Scheimpflug imaging provides quantitative assessment of opacity. Figure 13.4

The latent period
- Dose-related: latency gets shorter with increasing dose
- Average latency: 8 years for 2.5-6.5 Gy, 4 years for 6.51-11.5 Gy
- Latency can be much longer (~50 years) for lower doses (A-bomb survivors).
Dose-response relationship for cataracts in humans
- Historically categorized as a tissue reaction (deterministic effect) with a dose threshold.
- Threshold initially thought to be 2 Gy (single exposure) or 5-8 Gy (fractionated or prolonged exposure) based on early work by Cogan, Merriam and Focht, which involved the study of a limited number of individuals (mostly elderly patients receiving radiotherapy as a treatment for cancer)
- A-bomb survivor study by Nerrishi et al. (2007) shows increased risk for surgery-requiring cataracts with dose, odds ratio 1.39 statistically significant at 1 Gy.
- Recent evidence (A-bomb survivors, astronauts, Chernobyl workers, medical staff) suggests effects at lower doses and questions the high threshold.
- ICRP (2011) revised the threshold dose to 0.5 Gy from 2 Gy or 5-8 Gy.
- Occupational lens exposure limits subsequently lowered. ICRP recommends an average of 20 mSv per year over 5 years, with no single year exceeding 50 mSv. NCRP recommends an occupational exposure limit of 50 mGy per year.
WBRT, ocular MALToma 에서 꼭 설명을 드린다.
conjunctival MALToma: lens block을 사용하면 상당히 발생률이 낮아진다 (~2%)