Introduction
Virology and etiology
Hepatitis A
Hepatitis B
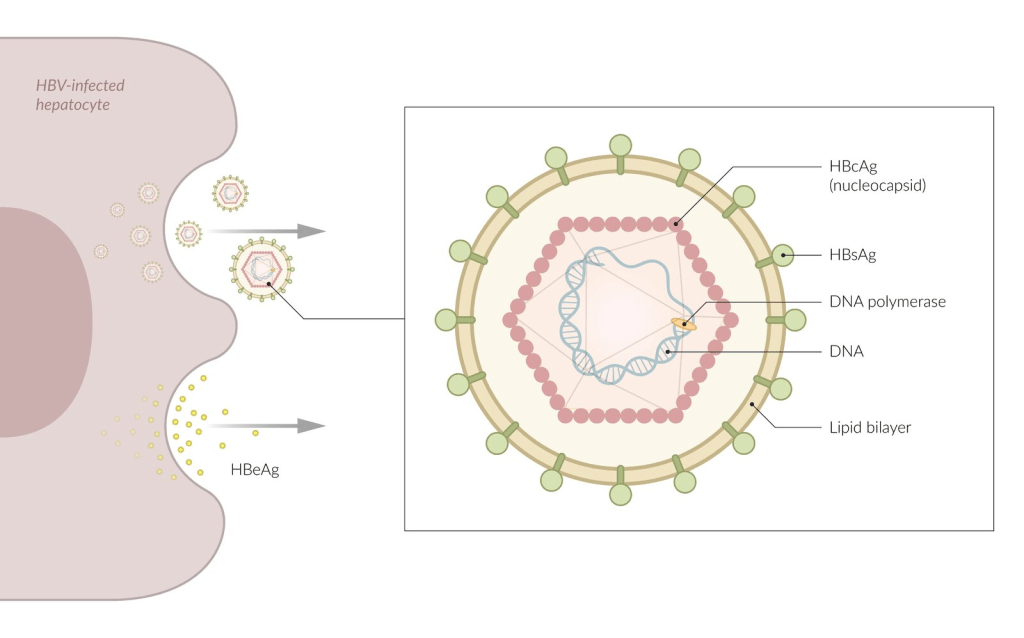
Viral proteins and particles
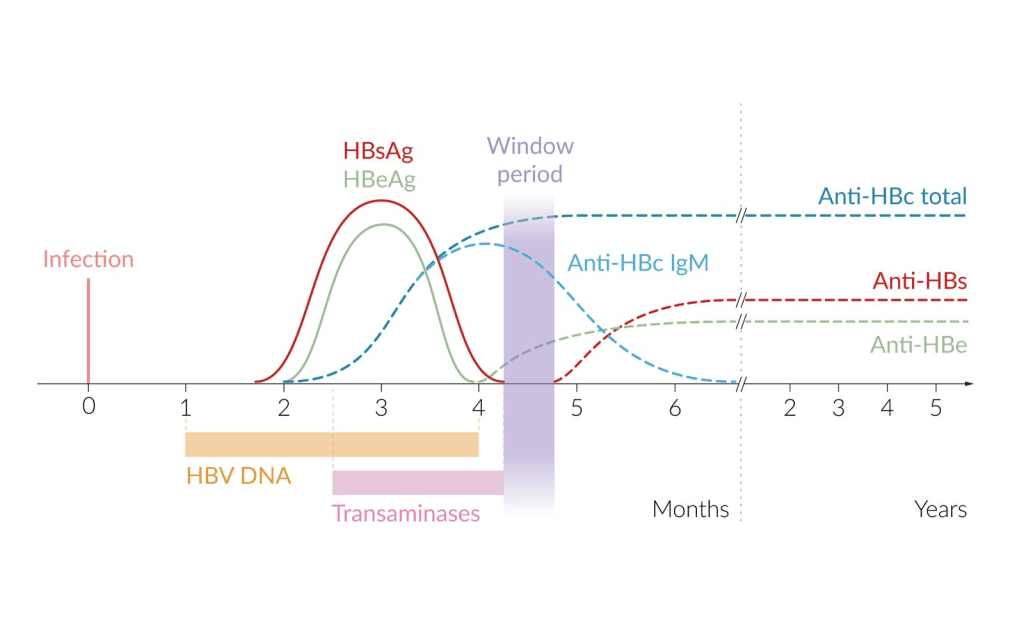
Serologic and virologic markers
HBV has no direct cytotoxic effect, but the presence of viral HBsAg/cAg on the cell surface stimulate the host?s cytotoxic CD8+ T lymphocytes to destroy infected hepatocytes.
HBsAg ???? ?? ??? – mutation?? ?? ??? ??? ???? ? HBV DNA
HBs? Ag, Ab? ?? ??? – ?? ?? ???? or HBV? ?? or ???? Ab? x
Molecular variants
Extrahepatic sites
Hepatitis D
Hepatitis C
Hepatitis E
Pathogenesis
Hepatitis B
Hepatitis C
Extrahepatic manifestations
by immune complex-mediated tissue damage
Serum sickness syndrome
related to the deposition in tissue blood vessel walls of HBsAg–anti-HBs circulating immune complexes, leading to activation of the complement system and depressed serum complement levels.
Glomerulonephritis
Essential mixed cryoglobulinemia (EMC)
The association with HBV is limited.
A substantial proportion has chronic HCV infection.
Treatment
- Mild disease
- e.g., only nonulcerating skin lesions ± mild neuropathy
- Direct-acting antiviral (DAA) therapy
- Severe disease
- e.g., renal failure requiring hemodialysis (d/t RPGN)
Pathology
Epidemiology and global features
Hepatitis A
Hepatitis B
Hepatitis D
Hepatitis C
Hepatitis E
Clinical and laboratory features
Symptoms and signs
- Serum sickness-like syndrome
- Fever
- Pruritic urticarial rash
- Arthralgia
- Lymphadenopathy
- Polyarteritis nodosa
- Beads on a string appearance
- Membranous, MPGN
Laboratory features
| HBsAg | ANTI- HBs | ANTI- HBc | HBeAg | ANTI- HBe | INTERPRETATION |
| + | – | IgM | + | – | Acute hepatitis B, high infectivity |
| + | – | IgG | + | – | Chronic hepatitis B, high infectivity |
| + | – | IgG | – | + | 1. Late acute or chronic hepatitis B, low infectivity 2. HBeAg-negative (?precore-mutant?) hepatitis B (chronic or, rarely, acute) |
| + | + | + | +/- | +/- | 1. HBsAg of one subtype and heterotypic anti-HBs (common) 2. Process of seroconversion from HBsAg to anti-HBs (rare) |
| – | – | IgM | +/- | +/- | 1. Acute hepatitis Ba 2. Anti-HBc ?window? |
| – | – | IgG | – | +/- | 1. Low-level hepatitis B carrier 2. Hepatitis B in remote past |
| – | + | IgG | – | +/- | Recovery from hepatitis B |
| – | + | – | – | – | 1. Immunization with HBsAg (axer vaccination) 2. Hepatitis B in the remote past (?) 3. False-positive |
Prognosis
HBV
- 95%: acute hepatitis? ?? completely resolve
- 4-5%: develop chronic hepatitis
- 50-80% remain stable
Complications and sequelae
Fulminant hepatitis
Etiology
HBV? m/c cause, ??? HDV? ?? ?
? ? drug toxicity, HAV, autoimmune hepatitis, ischemia, Wilson disease, and malignant infiltration of the liver.
Pathophysiology & Diagnosis
- Severe acute liver injury without cirrhosis or underlying liver disease.
- The diagnosis requires:
- Elevated aminotransferases (often >1,000 U/L)
- Signs of hepatic encephalopathy (HE)
- Impaired hepatic synthetic function (defined as INR ?1.5)
?? ??? ?? 8? ?? ??? ??, ????? ???? ?. -> ?? ????? ??? ??, ???.
Prognosis
Prognostic factors
???? ?? ??
Bilirubin ??? ?
PT ??
??
??? ?? AST, ALT, albumin, virus titer
Management
????? glucocorticoid, prostaglandin, ???? ?. ???? ??? ?? ??.
Differential diagnosis
Treatment
Prophylaxis
Hepatitis A
Hepatitis B
???? 3? ? ???? ???? ??? protective effect? ??? ?????/???? booster ?? ?? ??.
?? ? ??
- Perinatal exposure
- HBIG 0.5mL 1? IM + 12hr ?? vaccine (3?)
- Direct percutaneous/transmucosal exposure
- HBIG 0.06mL/kg IM + 1? ?? vaccine
- Booster: ?????? ?? ??
- Direct sexual contact
- HBIG 0.06mL/kg IM + 2? ?? vaccine