INTRODUCTION
ASSESSMENT OF ILLNESS SEVERITY
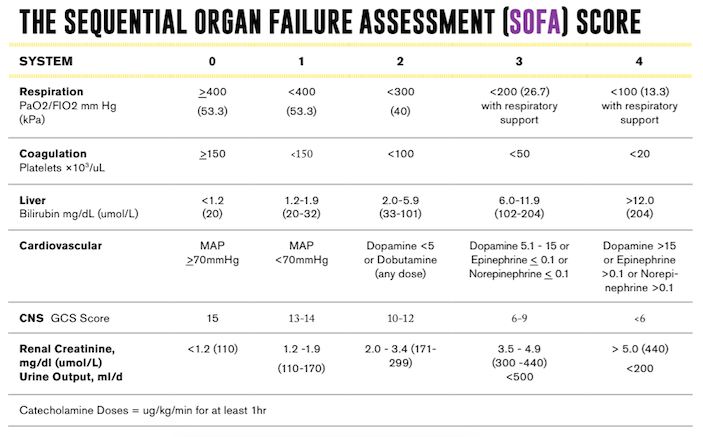
THE SOFA SCORING SYSTEM
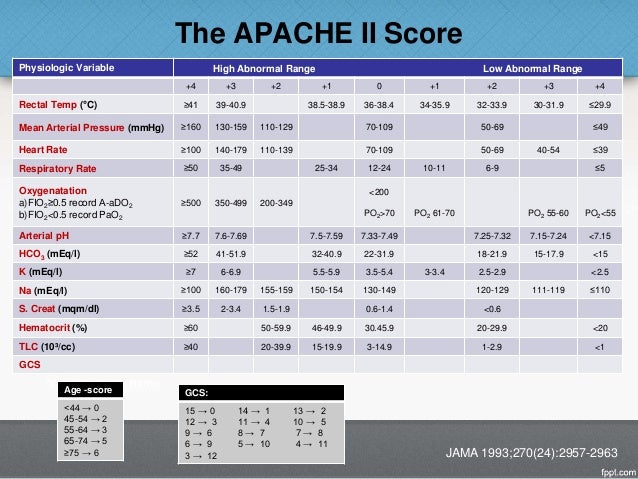
THE APACHE II SCORING SYSTEM
THE SAPS SCORING SYSTEM
SHOCK
INITIAL EVALUATION
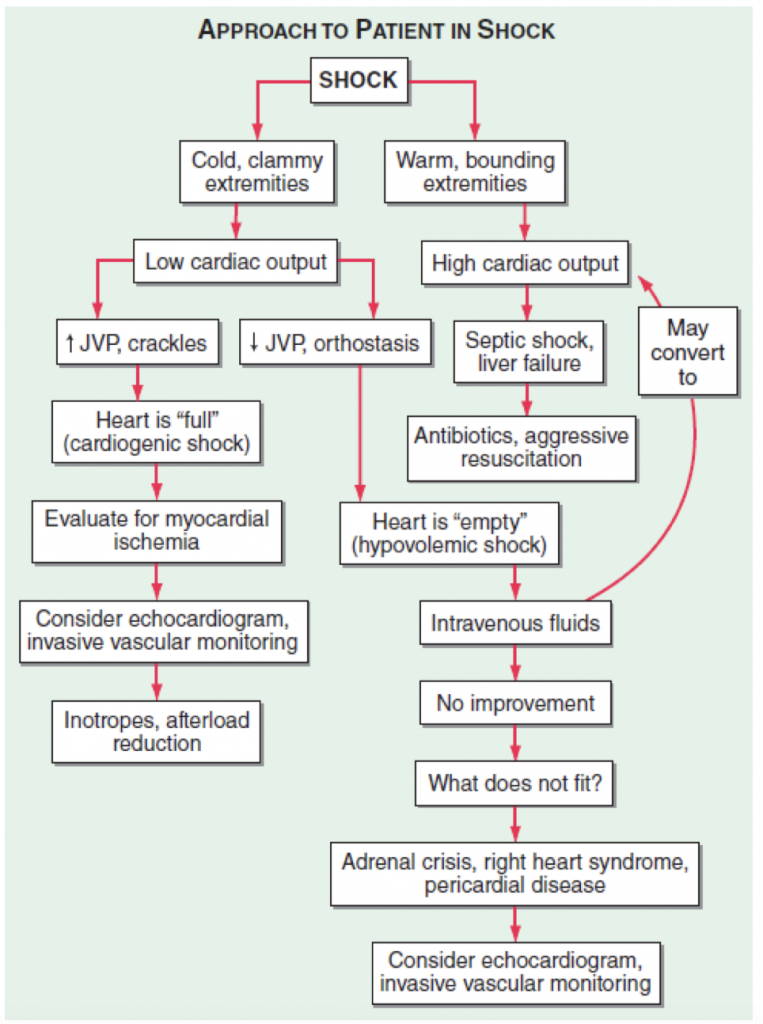
FIGURE 293-2
Approach to the patient in shock.
RESPIRATORY FAILURE
TYPE I: ACUTE HYPOXEMIC RESPIRATORY FAILURE
occurs with alveolar flooding and subsequent intrapulmonary shunt physiology.

FIGURE 293-5
Pressure-volume relationship in the lungs of a patient with acute respiratory distress syndrome (ARDS). At the lower inflection point, collapsed alveoli begin to open and lung compliance changes. At the upper deflection point, alveoli become overdistended. The shape and size of alveoli are illustrated at the top of the figure.
TYPE II: HYPERCAPNEIC RESPIRATORY FAILURE
consequence of alveolar hypoventilation and results from the inability to eliminate carbon dioxide effectively.
TYPE III: LUNG ATELECTASIS
- most common pulmonary complications in the first 72 hours after surgery
- Patients subsequently develop regional alveolar collapse and hypoxemia from a V/Q mismatch as well as a right-to-left pulmonary shunt in the area of atelectasis.
- To compensate for the resulting hypoxemia, the patient hyperventilates to increase ventilation of the noncollapsed alveoli and often develops respiratory alkalosis. Hypoxemia due to a right-to-left pulmonary shunt cannot be improved by 100% O2 delivery; instead, alveolar recruitment needs to be facilitated using adequate analgesia and lung expansion maneuvers.
TYPE IV: METABOLIC DEMANDS
hypoperfusion of respiratory muscles in patients in shock.
CARE OF THE MECHANICALLY VENTILATED PATIENT
MULTIORGAN SYSTEM FAILURE
MONITORING IN THE ICU
PULSE OXIMETRY
RESPIRATORY SYSTEM MECHANICS

FIGURE 293-6
Increased airway resistance with auto-PEEP. The top waveform (airway pressure vs. time) shows a large difference between the peak airway pressure (80 cmH 2 O) and the plateau airway pressure (20 cmH 2 O). The bottom waveform (flow vs. time) demonstrates airflow throughout expiration (reflected by the flow tracing on the negative portion of the abscissa) that persists up to the next inspiratory effort.