from Novac, Chapter 36 Cervical and Vaginal Cancer
Cervical cancer
Introduction
SCC(80%), adenocarcinoma(15%); both associated with HPV
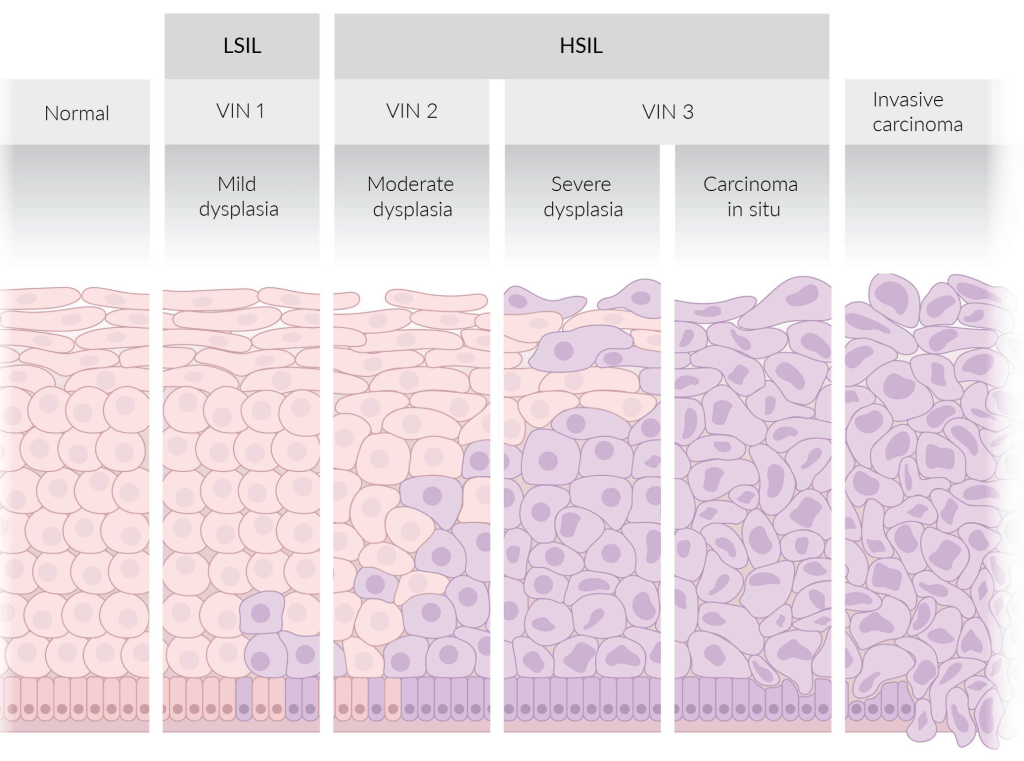
CIN to carcinoma, on average, takes 10-20 years.
Pap smear: limited efficacy in screening for adenocarcinoma
Clinical presentation
??? ??. Maybe ??? ??, ???? ??.
??? ????? ? ? ?? ???? ??? ?? X ??? ??? ????.
Staging
Base line study
Hx, P/E, IVP, barium enema, X-rays
Something I can see directly (~scopy, HSG, Bx, ECC, conization)
| 2018 FIGO stage | Sub-stage | Definition | Surgery | If wishes to conceive | Chemo/radiotherapy |
|---|---|---|---|---|---|
| Stage 1 | 1A1 | D <3mm, W <7mm | Simple hysterectomy | Conization or LEEP | X |
| 1A2 | D 3-5mm, W <7mm | Radical hysterectomy + Pelvic LND If have any high-risk factors (margin +, LN meta, parametrium), post-op CCRT | Conization or LEEP | X | |
| 1B1 | D >5mm, W ≤2cm | Radical trachelectomy + Pelvic LND | |||
| 1B2 | D >5mm, W 2-4cm | ||||
| 1B3 | D >5mm, W >4cm | pre-op CCRT | |||
| Stage 2 | 2A1 | ~Uterus, S ≤4cm | |||
| 2A2 | ~Uterus, S >4cm | pre-op CCRT | |||
| 2B | Parametrial invasion | Adjuvant hysterectomy | CCRT + palliative CTx | ||
| Stage 3 | 3A | Lower 1/3 of vagina | |||
| 3B | Pelvic wall +/- hydronephrosis or nonfunctioning kidney | ||||
| 3C1 | Pelvic LN only | ||||
| 3C2 | Para-aortic LN | ||||
| Stage 4 | 4A | Adjacent organs (bladder or rectum) | |||
| 4B | Distal organs |
65???? screening
??? CIN2 ??? ??? ??? ??? screening ??
???? ?? 20?? ? ?? ??
# ??? ??
- After radical hysterectomy -> RTx
- RTx -> surgical management
- Surgery nor RTx -> palliative CTx
- CCRT -> CTx +/- RTx
# ?? ? ??????
- IA1: ??? ?? ? 6? ? ????? ?? ??.
Vaginal cancer
Squamous cell carcinoma SCC
Etiology
- Risk factors
- Age >60
- HPV-16, 18 infection
- Tobacco use
In utero DES exposure(clear cell adenocarcinoma only)
- Usually 2? to cervical SCC.
- 1? vaginal carcinoma is rare.
- Upper 1/3 of the vaginal on the post.
- Wall – coitus? ???. Field theory
Clinical features
- Vaginal bleeding
- Malodorous vaginal discharge
- Irregular vaginal lesion
Management
- 1-2?
- ??? ??
- 4? with fistula
- ???????? (pelvic exenteration)
- ???
- RTx only
Clear cell adenocarcinoma
Malignant proliferation of glands with clear cytoplasm
Rare, but feared, complication of DES-associated vaginal adenosis.
Embryonal rhabdomyosarcoma
Malignant mesenchymal proliferation of immature skeletal muscle; rare
Presents as bleeding and a grape-like mass protruding from the vagina or penis of a child (usually<5 yrs of age); also known as sarcoma botryoides.
- Rhabdomyoblast, the characteristic cell
- Exhibits cytoplasmic cross-striations: spindle-shaped cells
- Immunohistochemical staining for desmin and myogenin.
Vulvar cancer
Management
Surgical therapy
- Radical/simple partial vulvectomy (first line)
- +/- SLNB
- +/- inguinofemoral lymphadenectomy: recommended in
- Recommended if SLNB+ or tumors >4cm or multifocal
Radiotherapy
- If surgical therapy is not feasible or if RM+
- +/- inguinofemoral RT
- may be considered for inguinofemoral metastases