Anatomy
Epidemiology, Presentation, and Management
- Rarity
- 2% of adult and 4.5% of pediatric gynecologic malignancies.
(~90%: metastasis from cervix/uterus)
- 2% of adult and 4.5% of pediatric gynecologic malignancies.
- Histology
- (Adults) 80-95% are Squamous Cell Carcinoma (SCC), mostly HPV-associated
- (Pediatric) Embryonal Rhabdomyosarcoma (RMS) and Yolk Sac Tumour (YST).
- Survival
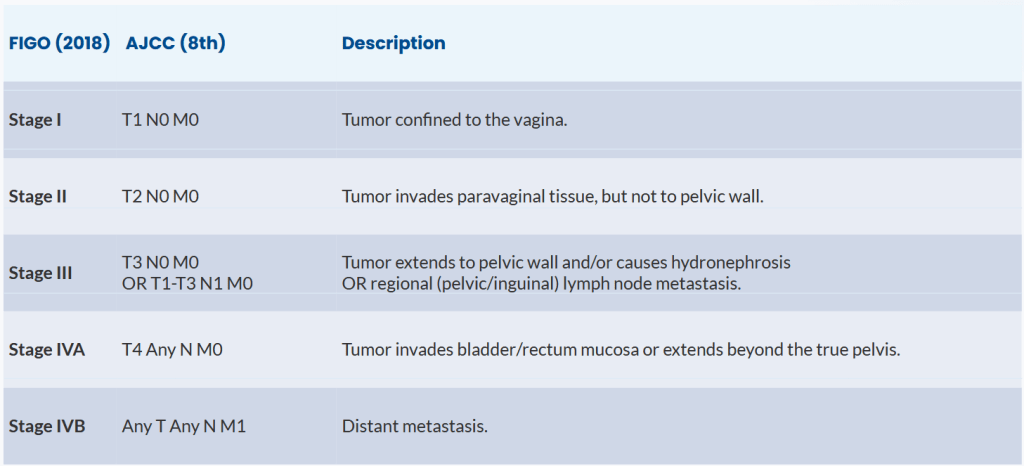
- 5-years OS: 77%, 52%, 42%, 20% and 13% for stages I, II, III, IVA and IVB
1940-70년대에 임신 중 DES 복용 후 adenoca. 생기는게 사회적인 문제가 된 적이 있다.
Vaginal Intraepithelial neoplasia (VAIN)
Squamous Cell Carcinoma
Clinical Presentation
Patterns of Lymphatic Drainage
Staging
Diagnostic Workup
Risk Factors
Prognostic Factors
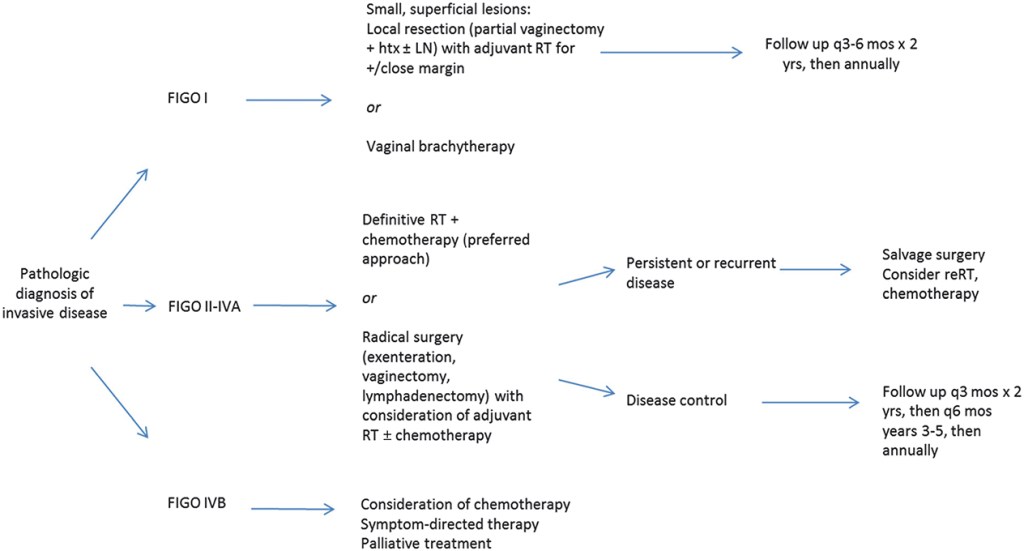
Treatment Options
- Stage I (T1N0)
- Primary Surgery: if small (<2cm), R0 feasible, low morbidity
- Primary (C)RT: combination of cisplatin-CCRT+brachy is recommended.
- Locally Advanced (T2-4 or N1)
- Definitive platinum-based CCRT, consolidated by a brachytherapy boost
Melanoma
Treatment Options
genital melanoma는 상당한 난치병.. Carbon의 적응증에 해당된다.
Sarcoma
Prognostic Factors
Treatment Options
Outcomes
Malignant Mixed Mullerian Tumors
Clear Cell Adenocarcinoma
Epidemiology
Risk Factors
Histopathology
Clinical Presentation
Prognostic Factors
Treatment Options
Other Adenocarcinomas
Lymphoma
Small Cell Carcinoma of the Vagina and Other Rare Histologies
Pediatric vaginal tumors (RMS, YST) are highly chemosensitive. Primary goal is organ preservation, and initial radical surgery should be avoided.
Radiotherapy Techniques
EBRT
Dose: 45-46 Gy in 1.8-2.0 Gy/fx.
Chemo: Concurrent weekly Cisplatin (40 mg/m²).
Timing: Overall Treatment Time (OTT) < 7-8 weeks.
Technique: IMRT and IGRT are recommended.
<Target volume>
Standard: Primary tumor, entire vagina, paravaginal space,
parametria, pelvic LNs (iliacs, obturator, presacral).
Lower 1/3 Tumors: Must include inguino-femoral LNs.
N1 Disease: Boost nodes to 55-60 Gy EQD2 (SIB or
sequential); consider para-aortic field
3D Conformal Treatment
IMRT
Brachytherapy
IGABT (Image-Guided Adaptive Brachytherapy) is recommended, preferably MRI-based
Applicator
- Cylinder, mold, or combined intravaginal/interstitial.
- Vaginal cylinder로 치료하기에는 적절한 dose를 cover하기에 어려운 경우가 많다.
- Insertstitial (needles) is required residual tumors >7mm thick or with paravaginal disease.
Dose
- Total Dose (D90 for CTV-T_HR): ≥ 75-85 Gy EQD2 (Combined dose from EBRT + BT)

Intracavitary Brachytherapy: LDR
Intracavitary Brachytherapy: HDR
Interstitial Brachytherapy
Brachytherapy Versus External Beam Boost
Treatment Toxicity and Management
Patterns of Failure
General Management, Treatment Options, and Outcomes: Special Scenarios
The Post-hysterectomy Patient
History of Prior Pelvic Radiation
Carcinoma of the Neovagina
Salvage Therapy for Recurrent or Persistent Disease
Palliative Therapy
Follow-Up
70-80% of relapses occur within 2 years
Years 1-2: Every 3-4 months
Years 3-5: Every 6-12 months
Routine cytology is not recommended