I. Cells and tissues
1. Effects of radiation on normal tissue
- cell killing (most)
- radiation-induced inflammatory cytokines: N/V, fatigue, Acute edema, Somnolence
2. Radioresponsiveness of a tissue
- inherent sensitivity of cells
- kinetics of the tissue
- the way cells are organized in that tissue
3. Radioresponse of tissues
: functioning differentiated cells < dividing cells
II. Early and late effects
| Early effect | Late effect | |
| α/ß ratio | About 10 Gy | About 2 Gy |
| Fx | More sensetive | |
| Tissue | Rapidly proliferating | Slowly proliferating |
| Skin, GI epithelium, hematopoietic | Lung, kidney, heart, liver, CNS | |
| Cause | Death of large amount cells | Vascular damage loss of parenchymal cells |
| Onset | Days~ weeks | Months ~ years |
| Repair | Rapidly, maybe completely | Never completely reversible |
* Consequential late effect: late effect consequent to a persistent severe early effect
ex) fibrosis, necrosis of skin consequent to desquamation and acute ulceration
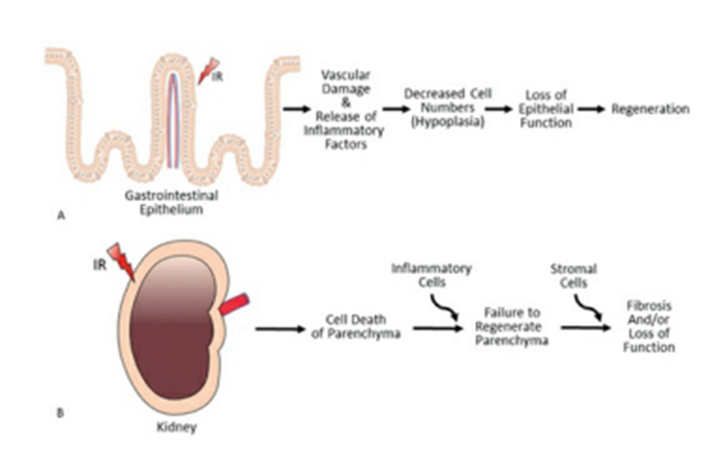
III. Functional subunits (FSUs) in normal tissue
1. Structurally defined FSUs
- kidney, liver, lung, exocrine organs
- small self-contained entity independent of its neighbors
- tissue survival depends on the No & radiosensitivity of clonogenic cells within FSU
2. Structurally undefined FSUs
- skin, mucosa, spinal cord
- clonogenic cells can migrate – repopulation of a depleted FSU
3. Tissue rescue unit
: minimum number of FSUs required to maintain tissue fuction
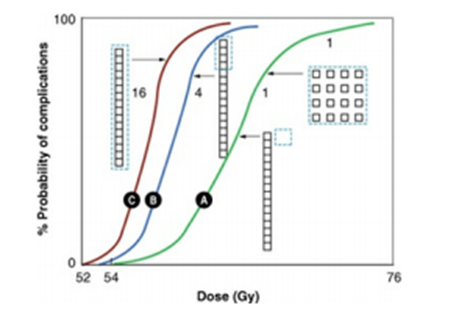
IV. The volume effect in radiotherapy : tissue architecture
1. Tolerance dose
: dose that produces an acceptable probability of treatment complication
2. Spatial arrangement of the FSUs in the tissue
- serial organization
- the integrity of each FSUs is critical to organ function (ex. spinal cord)
- binary response with a threshold dose
- volume effect
- parallel organization
- ex) kidney, lung: radiosensitive but small volumes can be treat to higher dose -> d/t functional reserve capacity
- graded response with a threshold volume
V. Radiation pathology of tissues
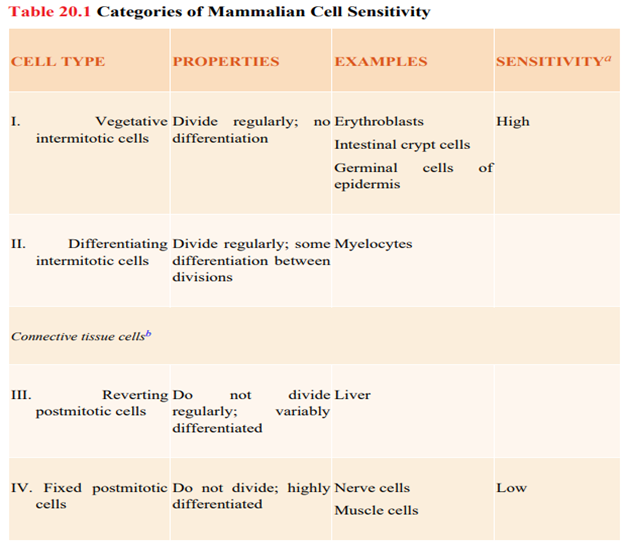
1. Casarett’s classification of tissue radiosensitivity
: based on histologic observation of early cell death
2. Michalowski’s H- and F-type populations
- H-type population (hierarchical): hematopoietic BM, intestinal epi, epidermis
- stem cells: crypt cells in the intestinal mucosa
- functional cells: circulatory granulocyte, cells that make up the villi of the intestinal mucosa
- mature partially differentiated cells: erythroblast and granullblasts
- F-type population (flexible): liver, thyroid, dermis
: rarely divide under normal conditions but can be triggered to divide by damage
no compartment, no strict hierarchy
* Many tissues are a hybrid of H-type and F-type
VI. Growth factors
- RT -> interleukin-1, linterleukin-6 ↑
- interleukin-1: radioprotectant of hematopoietic cells by increasing shoulder and D0
- Basic fibroblast growth factor: ↑ endothelial growth , ↓ apoptosis
-> protects microvascular damage (branching midsize capillary > nonbranching capillary)
- platelet-derived growth factor ß: ↑ vascular damage
- TGF-ß (transforming growth factor)
- : strong inflammatory response (ex. Pneumonitis)
- ↑ connective tissue growth, ↓ epithelial cell growth à fibrosis, vascular damage
- ↓ interleukin-1, TNF (tumor necrosis factor): ↑ hematopoietic tissue damage
- TNF
- : cytotoxic agent
- ↑ proliferation of fibroblast, inflammatory cell, and endothelial cell
- protect hematopoietic cells, sensitizes tumor cells to radiation
- serum consentration: correlate with severity of pneumonitis, hepatic dysfunction, renal insufficiency, and demyelination
VII. Specific tissues and organs (Table 20.2)
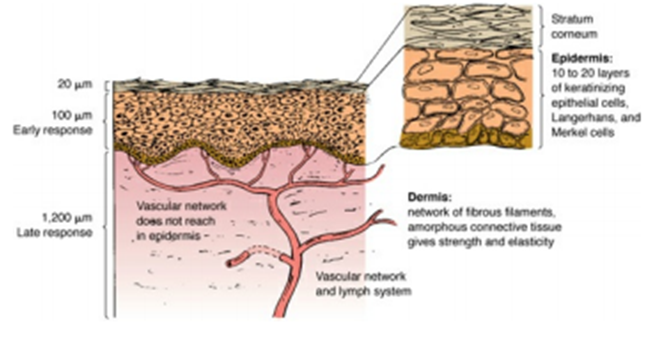
Skin
1. Epidermis: Early radiation reactions
It takes about 14 days from the time a newly formed cell from basal layer to the time it is desquamated from the surface
2. Dermis: Late radiation reactions
1~3mm thick
Vasculature of the dermis plays a major role in the radiation response
Few hours after doses greater than 5Gyà erythema
Orthovoltage -> Full dose is deposited in the superficial layer -> Erythema develops in the 2nd to 3rd week, followed bydry or moist desquamation
Megavoltage -> Dmax occurs at deep layer -> 60Gy or more are tolerate
Hematopoietic system
- 60% in the pelvis and vertebrae
- TBI
- 0.3 Gy leads to a reduction in the number of lymphocytes
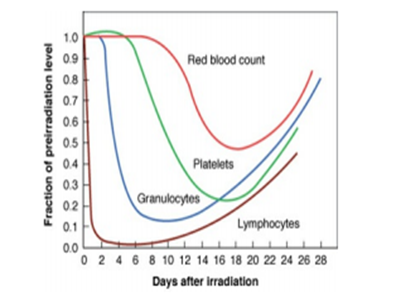
- General pattern of the blood counts after amodest dose of radiation (fig. 20.4): LGPR
- Partial body radiation
- Compensatory hyperplasia attempts to maintain the total production of blood elements at long bones, spleen, liver
- Doses greater than about 30Gy may cause permanent aplasia
- Chemotherapy agents
- The marrow of patients irradiated to a large volume is always more sensitive to cytotoxic drugs because a greater proportion of stem cells are dividing actively
High-yield…
Lymphoid tissue and the immune system
- Lymphocytes are very radiosensitive, because of apoptosis. B cell more sensitive than T cell
- Total body dose 3.5~4 Gy inhibits the immune response
Digestive tract
Oral mucosa
- 1st week: asymptomatic focal hyperemia and edema
- 2nd week: increasing pain and loss of desire to eat, early desquamative mucositis occurs.
- 3rd week: mucositis and swelling with depletion of gland secreation. Diffulty in swalling
- 4th week: progression of signs
- 5th week maximum radiation damage apparent.
- In 2 to 4 weeks complete resolution
- Xerostomia. TD5/5 32Gy, TD50/5 46Gy
Esophagus
- 10 to 12 days after therapy, substernal burning with pain and swalling
- Late effects are related to the muscle layer
Stomach
- Delayed gastric emptying and epithelial denudement: early radiation effectPeptic ulcer: more than 40Gy
Small and large intestines
- Acute mucositis: interruption of treatment for a few days alleviates the symptom
- Late effect: fibrosis and ischemia
- Tolerance dose for small intestine 50 Gy, rectal tolerance 70Gy
Lungs
The most sensitive of late-responding organ
- Acute pneumonitis at 2 to 6 month
- Fibrosis: several months to year
- Difficulties in respiratory function: volume irradiated, dose, fraction size
- a/b: 3Gy (particulary sensitive to fractionation)
- Most sensitive to late response
Kidneys
- Radiosensitive late-responding organ
- 30Gy/15fx -> Nephropathy with arterial HTN, anemia
- Increasing treatment time does not allow higher doses to be tolerated
- FSUs are arranged in parallel, with each containing only about 1,000 stem cells
Liver
- Fatal hepatitis may result from only 35 Gy if the whole organ is irradiated
- Parenchyma: parallel, Hilum: serial
Bladder epithelium
- low cell renewal rate / lifespan of superficial cell: several months
- frequency increases in parallel with bladder damage and loss of surface cells
- Late effect: fibrosis, reduction in bladder capacity
Central and peripheral nervous systems
Brain
- Cells
- neurons: nonproliferating end cells in adults
- glial cells: slow turnover, small stem-cell compartment (1%)
- vascular endothelial cells: slow turnover, rapid proliferation after injury
- < 6mo: transient demyelination (somnolence syndrome), leukoencephalopathy
- Radiation necrosis: 6mo ~ 2 to 3 years
Spinal Cord
- Lhermitte’s sign: demyelating injury, months~a year, reversible, 35 Gy
- Late damage: demyelination and necrosis of white matter (6-18 mo), Vasculopathy (1-4 years)
- TD5/5 50 Gy(10cm), 55 Gy(5cm) TD50/5 70 Gy
- Serially arranged FSU -> the probability of a myelopathy depends critically on the length irradiated for very small lengths, but once the length of the field exceeds a few centimeters, the treatment volume has little effect
- Neurotoxic chemotherapy agents: methotrexate, cis-platinum, vinblastine, AraC
- Animal data: about 2years, most of the damage repaired.
Peripheral nerves:
more radioresistant (few quantitative data),TD5/5 60 Gy (2 Gy/fx)
Genital
Testis
- germinal cells: radiosensitive, stem cell~ spermatozoa 74days
- 0.1 Gy: temporary reduction in the number of spermatozoa
- 0.15 Gy: temporary sterility
- 2 Gy: azoospermia for years
- 6-8 Gy (2 Gy/fx): permanent azoospermia
- Leydig cells: secrete testosterone, radioresistant
Ovaries
radiosensitive, D0 0.12 Gy, immediate sterilization, menopause
Female genitalia
- vulva: tolerance dose 50-70Gy
- vagina
- acute: erythema, moist desquamation, mucositis -> 3~6months
- Gross abnormalities: pale color, thin atrophic mucosa, inflammation, necrosis
- Tolerance dose: 90 Gy (~ulceration), 100Gy (~fistula)
- Uterus
- ICR: Cx, uterus dose 200Gyà atrophy of the endometrial gland and stroma
Blood vessels and the vascular system
- denudation of surface of vessels à thromboses, capillary necrosis
- loss of muscular fibers à replaced by collagen fibers: blood flow ↓
- capillary 40 Gy, artery 50 ~ 70Gy, vein most resistant
Heart
- intermediate tolerance, a/b ratio = 1Gy
- Acute pericarditis: m/c, > 1yr, transient pericarditis~cardiac constriction
- 20Gy (>50% volume)
- fractionated 45-50Gyà 11% incidence
- Acute pericarditis: m/c, > 1yr, transient pericarditis~cardiac constriction
- Cardiomyopathy: dense and diffuse fibrosis, many years
- In some Hodgkin disease (30Gy to most of the heart)
- Adriamycin (doxorubicin): ↑ severity of radiation-induced complication
Bone and cartilage
- Children: growing cartilage
- 10Gy can slow growth
- 20Gy: deficit in growth is irreversible
- damage ↑: higher dose, younger age (esp. <2 years)
- Adult
- Osteonecrosis: lower maxilla, large volume – TD5/5 50~60 Gy, TD50/5 70Gy
- Fracture of humeral and femoral head – TD5/5 52 Gy, TD50/5 65 Gy
VIII. QUANTEC, LENT and SOMA
- QUANTEC (2010): QUantitative Analysis of Normal Tissue Effects in the Clinic
- guideline on dose-response relationships in normal tissues
2) LENT, SOMA
- EORTC, RTOG (1992) – LENT conference: SOMA classification for late toxicity
- LENT: Late Effects of Normal Tissue
- SOMA: Subjective, Objective, Management criteria with Analytic laboratory and imaging procedures
QUANTEC (Table 20.3), SOMA (Table 20.4-20.6)
IX. Application of stem cells to regenerate radiation sensitive organs –salivary gland regeneration
Salivary gland: radiosensitive organs – apoptotic cell death
Autologus stem cell transfer
- Mouse model
invitro culture of salivary stem cell -> reinjected after irradiation
à repopulate the salivary gland and increased the salivary production - Limitation
- in vitro culture: needs at least for several months, spontaneous differentiation must be prevented
- radiation induced fibrosis