Cardiovascular Disorders
Physiologic considerations in pregnancy
Cardiovascular physiology
Ventricular function in pregnancy
- ?HR & blood volume
- ?Transmitral gradient and left atrial pressure (at rest and during exercise)
- Systolic ejection murmur
- Peripheral edema
- Respiratory adaptation
- Progesterone induces ?minute ventilation through an increase in tidal volume, but the respiratory rate is unchanged.
- The enlarging uterus ? diaphragm to be elevated ? ?FRC
Diagnosis of heart disease
Diagnostic studies
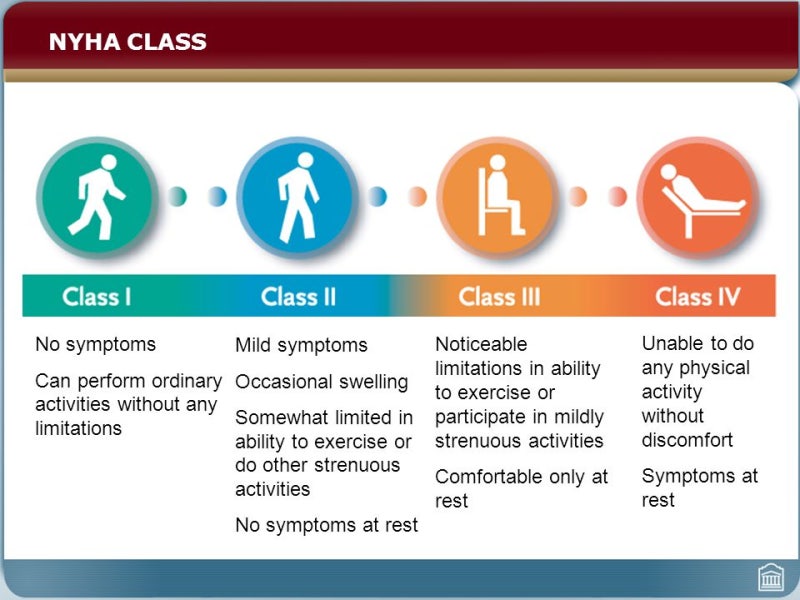
Classification of Functional Heart Disease
Preconceptional Counseling
Peripartum management considerations
Labor and Delivery
Analgesia and Anesthesia
Intrapartum Heart Failure
Puerperium
| NYHA I, II | Morbidity ?? ?? ????. Sepsis, bacterial endocarditis ??! |
| NYHA III, IV | ???? ?? ?? ?? bed rest ??? pregnancy interruption ??. Epidural ??, vaginal delivery > C-sec |
| Mitral insufficiency | ?? ??? ? ??? ??. ??? ??? x |
| Mechanical valve | ?? ? warfarin – ?? ? full heparin – ?? ?? heparin ?? ??? dual 6? – ? ? warfarin |
| Peripartum DCMP | CXR: Impressive cardiomegaly / EF < 45% |
| Infective endocarditis | Ampicillin 2g, or cefazolin or ceftriaxone 1g IV |
Surgically corrected heart disease
Valve Replacement before Pregnancy
Anticoagulation
Cardiac Surgery During Pregnancy
Pregnancy axer Heart Transplantation
Valvular heart disease
Mitral Stenosis
Physiologic changes often precipitate symptoms of fatigue, exercise intolerance, or dyspnea in previously asymptomatic patients with rheumatic mitral stenosis.
The loss of an effective “atrial kick” and decrease in diastolic filling times seen with AF and RVR further increases left atrial pressure, with dramatic worsening of pulmonary congestion/edema.
Mitral Insufficiency
Mitral Valve Prolapse
Aortic Stenosis
Aortic Insuwiciency
Pulmonic Stenosis
Congenital heart disease
ASD / VSD / AVSD
Persistent (Patent) Ductus Arteriosus
Cyanotic Heart Disease
Pregnancy axer Surgical Repair
Eisenmenger Syndrome
Pulmonary hypertension
Cardiomyopathies
HCMP
DCMP
Peripartum Cardiomyopathy
- Clinical features
- Onset of HF during last months of pregnancy or within 5 months following delivery
- LV systolic dysfunction with LVEF <45%
- Associated with mitral regurgitation
- Absence of other causes of HF
- Absence of heart disease prior to final month of pregnancy
- Dyspnea, peripheral edema, pulmonary edema with hyperventilation and respiratory alkalosis.
Other Cardiomyopathy Types
Heart failure
Diagnosis
Management
Infective endocarditis
Diagnosis and Management
Pregnancy
Endocarditis Prophylaxis
Arrhythmias
Bradyarrhythmias
Supraventricular Tachycardias
Ventricular Tachycardia
Prolonged QT-Interval
Diseases of the aorta
Aortic Dissection
Marfan Syndrome
Aortic Coarctation
Ischemic heart disease
Myocardial Infarction During Pregnancy
Pregnancy with Prior Ischemic Heart Disease
Chronic Hypertension
?? ???/????, MI, HF?? ??? Cix
Preeclampsia risk ?, placental abruption, FGR, preterm, perinatal death? ?
Anti HTN drug
Diurteics (?? thiazide), ACEI? ??!!
Methyldopa? ?? ??. Or hydralazine
Pulmonary Disorders
Asthma
PG, ergonovine
Pneumonia
CAP (community-acquired pneumonia)
- Etiology: S.pneumonia – m/c.
- Low threshold for admission – The presence of comorbidities (e.g., asthma, immunologic disorders, renal disease) warrants inpatient management.
Management
- In general: https://hsnow.net/infectious-diseases/h131-pneumonia/
- The approach to antibiotic therapy during pregnancy is the same as that for the general adult population,
- excluding potentially teratogenic medications, e.g.,: clarithromycin, fluoroquinolone, tetracycline
- Attenuated Influenza vaccine
Tb
HER – 3? 9?? ??. Mycin??, amikacin? CIx ????(TST+) – isoniazid 1? ?? Disseminated Tb? ?? ?? ??? ???? ??. ??? Tb? ? ???? ??? INH 1?. ????.
DVT
LMWH
Thromboembolic Disorders
Postpartum ovarian vein thrombosis
� Risk factors – Virchow�s triad
? Venous stasis (ovarian venous dilation)
? Hypercoagulability (hormone-mediated increase in clotting factors)
? Endothelial damage (interapartum vascular injury or uterine infection)
� Clinical presentation
? 1 week after delivery
? Fever & localized abdominal pain