Introduction
P2 C50 Hypercalcemia and Hypocalcemia
Parathyroid hormone
Chief cells regulate serum free (ionized) calcium via parathyroid hormone (PTH) secretion, which
Increases bone osteoclast activity, releasing calcium and phosphate
Increases small bowel absorption of calcium and phosphate (indirectly by activating vitamin D)
Increases renal calcium reabsorption (distal tubule) and decreases phosphate reabsorption (proximal tubule)
Increased serum ionized calcium levels provide negative feedback to decrease PTH secretion.
Parathyroid hormone-related protein PTHrP
Calcitonin
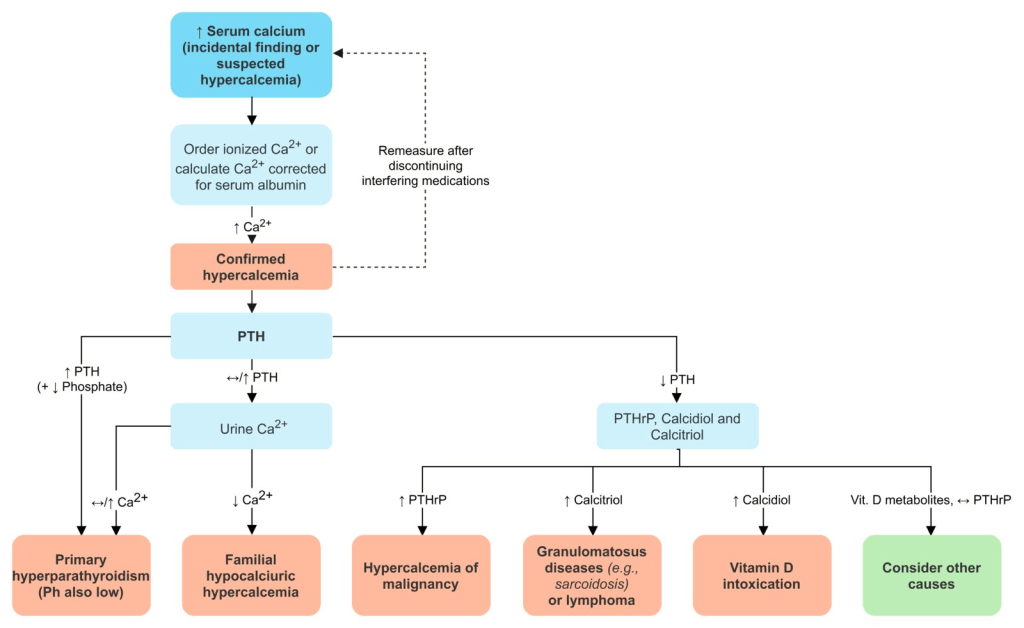
Hypercalcemia
Primary hyperparathyroidism
Solitary adenoma (80%) Chief cell parathyroid hyperplasia (15%, MEN1, 2A? ??)
Clinical presentation
50%? ???. ??? ?? ??? ?????�.
- Nephrolithiasis
- Calcium oxalate stones
- Nephrocalcinosis
- Metastatic calcification of renal tubules (Fig. 15.9), potentially leading to renal insufficiency and polyuria
- CNS disturbances (e.g., ??, ??, ??, ?? / ??? / ????)
- Constipation, peptic ulcer disease, and acute pancreatitis
- Osteitis fibrosa cystica
- Paracrine stimulation of osteoclasts by osteoblasts.
- Resorption of bone leading to fibrosis and cystic spaces filled with brown fibrous tissue.
- Cardiovascular
- Hypertension
- d/t ?renin secretion, sympathetic hyperresponsiveness, and peripheral artery vasoconstriction
- Treatment of PHPT usually results in normalization of BP
- LVH, arrhythmias, and vascular and valvular calcification.
- Hypertension
Diagnosis
Central: Sono
Distal: 99mTc sestamibi scan (SPECT)
PTH??? ??. ALP ?? (turnover ?), ??? ???? ?? (?? ???, ????)
Operation
P2 C38 Thyroid, Parathyroid, and Adrenal
Genetic defects associated with HPT
Other parathyroid-related causes of hypercalcemia
Genetic disorders causing hyperparathyroid-like syndromes
Familial hypocalciuric hypercalcemia (FHH)
- Pathophysiology
- Defective G-coupled Ca2+-sensing receptors(CaSRs) in multiple tissues (eg, parathyroids, kidneys).
- Higher than normal Ca2+ levels required to suppress PTH.
- Clinical manifestations
- Mild asymptomatic hypercalcemia
- Reduced urinary excretion of calcium (low UCCR)
- High normal or mildly elevated PTH.

Malignancy-related hypercalcemia
Vitamin D-related hypercalcemia
Hypercalcemia associated with high bone turnover
Hypercalcemia associated with renal failure
Severe secondary hyperparathyroidism
Renal insufficiency -> ?phosphate excretion.
? serum phosphate binds free calcium.
? free calcium stimulates all four parathyroid glands.
FGF23? ? VitD? ? Osteomalacia
Tertiary hyperparathyroidism
CKD? ???? ????? irreversible clonal outgrowth – refractory (autonomous) hyperparathyroidism
Aluminum intoxication
Milk-alkali syndrome
- Pathophysiology
- Excessive intake of calcium & absorbable alkali
- Renal vasoconstriction & decreased GFR
- Renal loss of sodium & water, reabsorption of bicarbonate
- Symptoms
- N/V, constipation
- Polyuria, polydipsia
- Neuropsychiatric symptoms
- Lab findings
- Hypercalcemia, metabolic alkalosis
- AKI, suppressed PTH, hypophosphatemia, hypomagnesemia
- Treatment
- Discontinuation of causative agent
- Isotonic saline followed by furosemide
Differential diagnosis: special tests
Treatment of secondary hyperparathyroidism
| Treatment | Target PTH level: 150~300pg/mL in CRF stage 5 |
| Phosphate binder (at emergency) | Ca carbonate/acetate: with risk of hypercalcemia Sevelamer hydrochloride: no risk of hypercalcemia |
| Active vitamin D | Direct action ? for refractory hyperparathyroidism (after revised hypeprphosphatemia) |
| Calcimimetics | Cinacalcet: increase sensitivity of Ca receptor (Used in refractory hypercalcemia) |
| VDR activator |
Differential diagnosis: special tests
Hypocalcemia
Symptom
Numbness and tingling (particularly circumoral)
Neuromuscular: muscle spasm, convulsion. May be elicited by Chvostek or Trousseau ? latent tetany
CNS: irritability, depression, psychosis
Functional classification
P ?? ??: Hypo-Mg2+, Active Vit.D deficiency
Treatment
Acute symptom
IV Ca gluconate
PTH absent
Vit D or calcitriol + high oral Ca / Mg ?? /
Renal stone ?? ?? thiazide on low sodium diet / PTH
PTH ineffective
Vit D or calcitriol + high oral Ca / Restriction of phosphate in diet
Pseudo-hypoparathyroidism
1A: PTH ? ?? kindey? ??? ??.
Albright�s hereditary osteodystrophy AHO
D/t defective Gs protein ? subunit causing end-organ resistance to PTH.
Autosomal dominant, must be inherited from mother d/t imprinting.
Short stature and short 4th and 5th digits.
Vit.D or calcitriol + high oral Ca
Pseudo-pseudo-hypoparathyroidism
AHO? ??? ????, Lab ??. ??? ?? ?? ??.
Occurs when defective Gs protein ? subunit is inherited from father.