Anatomy
Epidemiology
Human papillomavirus
E6 suppress p53
E7 affects Rb
HPV vaccination
Natural History and Patterns of Spread
CIN1 – 60% regression
CIN2 – 40% regression
Progression typicallyl takes 10 to 20 years
- Obturator lymph node
- Venous plexus, paracervical veins → hematogenous dissemination
Clinical Presentation
Diagnostic Workup
Conization/Loop excision
If <2cm on PET and MRI,
knife conization or lymphadenectomy for fertility preservation
Biopsy
Laboratory studies
Imaging studies
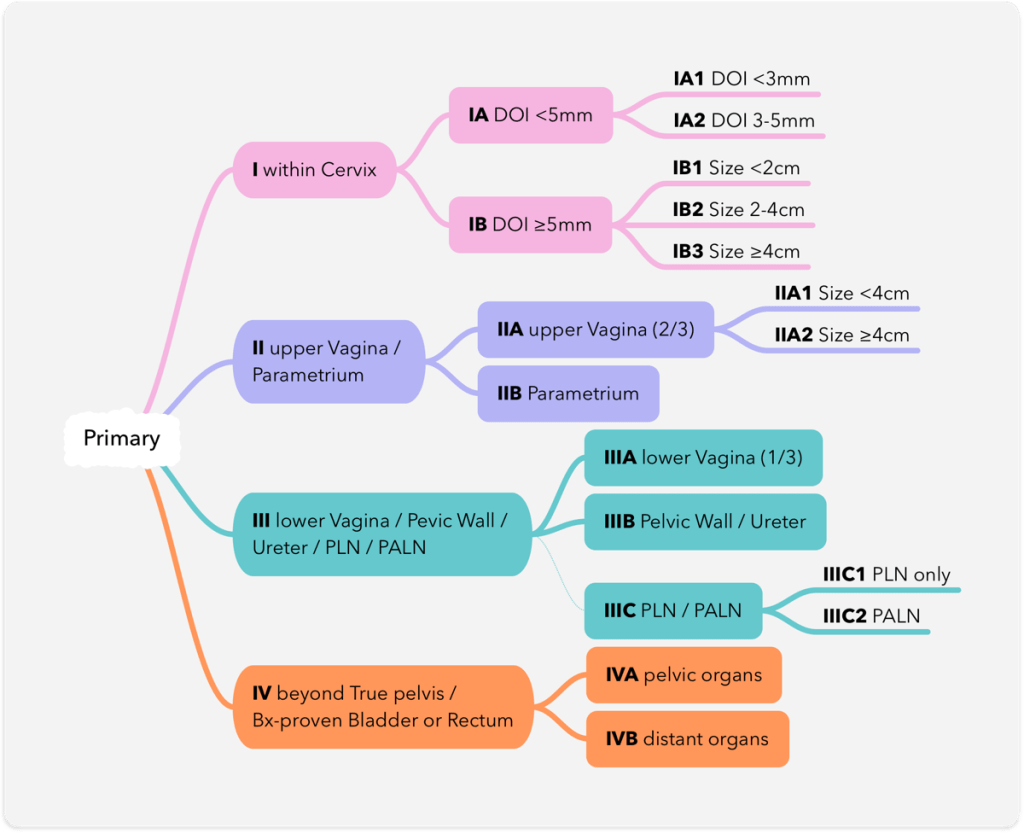
Staging
Pelvic LN+ rates
Pathologic Classification
Prognostic and Predictive Factors
Patient-related factors
- Age
- Race/Socioeconomic Status
General and medical factors
- Anemia and tumor hypoxia
- 수혈은 첫 RT dose 전에 시행되어야 한다.
- Other medical factors
Tumor factors
- HPV subtype
- Tumor volume
- Impact of histology on outcomes
Adenoca.는 원래 RT 반응이 좋지 않아 수술을 해야한다는 의견도 많다. 하지만 HP-associated adenoca는 좀 더 좋다.
Margin status after radical hysterectomy
Crude recur rates for any recurrence:
38% for RM+, 20% for cRM (<1cm), 11% for clear RM
Histologic grade
Lymph node ratio
Treatment duration
Biomarkers
- Angiogenesis and hypoxia
- Flow cytometry studies on DNA and growth fraction
- Apoptosis
- Cell cycle and cellular oncogenes
- Cytokeratin markers and the EGFR pathway
- Squamous cell carcinoma antigen (SCC-Ag) and carcinoembryonic antigen (CEA)
- CEA나 CA19-9의 증가는 advancec stage 또는 adenocarcinoma에서 더 흔했다
- Epstein-Barr virus, TGF, β-integrin, and other markers
- Cyclooxygenase-2 (COX-2)
- Hormonal Receptors
- Cancer genome atlas
Techniques Used for Treatment
Preinvasive Disease
Invasive disease
Surgical techniques
Simple conization
Radical trachelectomy
Selection criteria
- age <40
- stage IA1-IB1 with no nodal involvement on MRI and PET
- SqCC or ADC with lesion <2cm
- no LVSI on initial Bx
- No upper endocervical involvement
Types of hysterectomy
Pelvic exenteration
Pretreatment surgical nodal assessment
Surgical nodal debulking → RT
Sentinal lymph node biopsy
20% false-negative, 50% incidence of other pelvic metastasis
Ovarian transposition
32-88% ovarian preservation rate
Risk factors for ovarian metastasis → NOT a candidate for the ovarian transposition
- FIGO IA-IIB 대상 18,389 pts from 12 studies
- Pelvic LN involvement, parametrial, uterine corpus invasion
- FIGO IB-IIB 대상 🇯��
- ADC 5.31% vs SCC 0.79%
- SNUH retro , 625 pts with RH+BSO, 256 ovary preserved
- Non-SCC 7.9%, SCC 0.4%
- MVA에서 uterine invasion과 histology가 independent prognostic factor
- But non-SCC에서 preservation을 고려할 수 있겠다.
RT techniques
General Management
🇮 73 Uterine Cervix – General management
Brachytherapy
🇮 73 Uterine Cervix – Brachytherapy