Introduction

FIGURE 111-1 Immunoglobulin genetics and the relationship of gene segments to the antibody protein. The top portion of the figure is a schematic of the organization of the immunoglobulin genes, λ on chromosome 22, κ on chromosome 2, and the heavy chain locus on chromosome 14. The heavy chain locus is >2 megabases, and some of the D region gene segments are only a few bases long, so the figure depicts the schematic relationship among the segments, not their actual size. The bottom portion of the figure outlines the steps in going from the noncontiguous germline gene segments to an intact antibody molecule. Two recombination events juxtapose the V-D-J (or V-J for light chains) segments. The rearranged gene is transcribed, and RNA splicing cuts out intervening sequences to produce an mRNA, which is then translated into an antibody light or heavy chain. The sites on the antibody that bind to antigen (the so-called CDR3 regions) are encoded by D and J segments for heavy chains and the J segments for light chains.
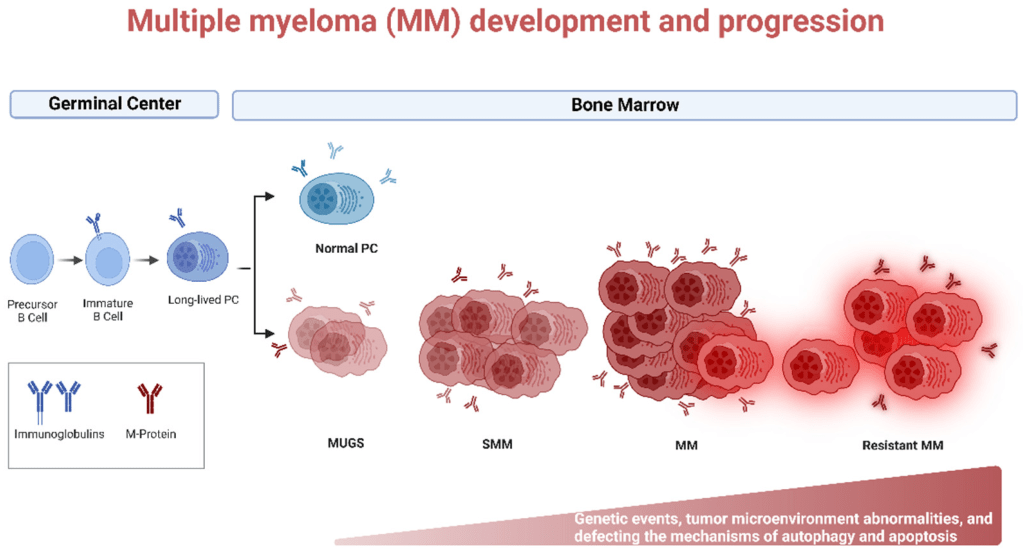

Monoclonal gammopathy(MGUS, pre-cancerous) -> MM / Waldenström
cf) heavy chain disease, cryoglobulinemia, amyloidosis
| MGUS | SMM | MM | |
| Plasma cells on BM Bx | <10% | 10-60% | >60% |
| Serum monoclonal protein (IgG or IgA) | <3g/dL | ≥3g/dL | |
| Myeloma defining event | NO | NO | YES |
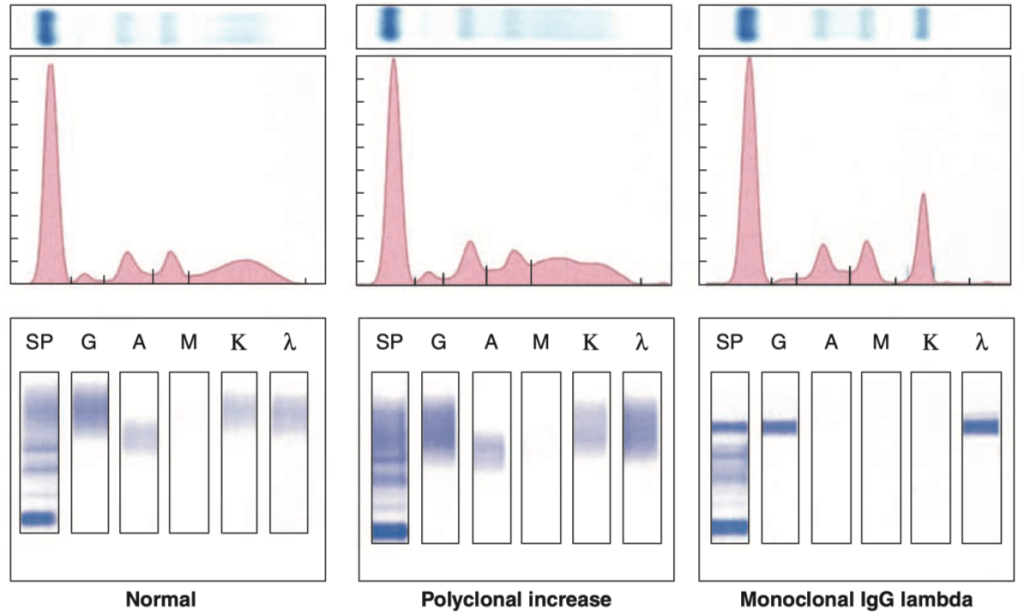
FIGURE 111-2 Representative patterns of serum electrophoresis and immunofixation. The upper panels represent agarose gel, middle panels are the densitometric tracing of the gel, and lower panels are immunofixation patterns. The panel on the left illustrates the normal pattern of serum protein on electrophoresis. Because there are many different immunoglobulins in the serum, their differing mobilities in an electric field produce a broad peak. In conditions associated with increases in polyclonal immunoglobulin, the broad peak is more prominent (middle panel). In monoclonal gammopathies, the predominance of a product of a single cell produces a “church spire” sharp peak, usually in the γ globulin region (right panel). The immunofixation
Multiple myeloma, MM
Definition
Most common primary malignancy of bone.
High serum IL-6 is sometimes present; stimulates plasma cell growth and immunoglobulin production
IgG(55%) > A(25%) > D > E, light chain
Etiology
Myeloma cells stimulate osteoclast maturation by producing RANKL and by destroying OPG
Inhibit osteoblast activity by secreting cytokines that block osteoblast function (e.g., IL-3, IL-7, Wnt pathway inhibitors)
Incidence and prevalence
Global considerations
Pathogenesis and clinical manifestations
- Bone pain with hypercalcemia
- Neoplastic plasma cells activate the RANK receptor on osteoclasts, leading to bone destruction.
- [A] Lytic, ‘punched-out’ skeletal lesions are seen on x-ray, especially in the vertebrae and skull; increased risk for fracture
- Elevated serum protein
- Neoplastic plasma cells produce immunoglobulin
- M spike is present on serum protein electrophoresis (SPEP), most commonly due to monoclonal IgG or IgA.
- ?Gamma gap; total protein and albumin difference
- Increased risk of infection
- Monoclonal antibody lacks antigenic diversity
- Infection is the most common cause of death in multiple myeloma.
- Pneumonia – S.pneumonia is the m/c.
- Urinary tract infection
- LIght cain
- Circulate in serum and deposit in tissues ? Primary AL amyloidosis
- Excreted in the urine as Bence Jones protein ? deposition in kidney tubules leads to risk for renal failure (myeloma kidney).
- Blood smear
- [B] Rouleaux formation of RBCs; increased serum protein decreases charge between RBCs
- [C] Numerous plasma cells with �clock-face� chromatin and intracytoplasmic inclusions containing immunoglobulin.
- Basophilic cytoplasm, well-developed Golgi apparatus (perinuclear paleness)
Diagnosis and staging
Diagnosis criteria by International Myeloma Working Group
- Histopathologic criteria
- BM biopsy: plasmatosis >10% OR
Bx-proven plasmacytoma (bony or extramedullary)
- BM biopsy: plasmatosis >10% OR
- At least 1 myeloma defining event
- CRAB criteria (end-organ damage)
- Calcium increased: >11 mg/dL or >1 mg/dL above the ULN
- Renal insufficiency: GFR < 40mL/min or Cr >2 mg/dL
- Anemia: Hb <10 g/dL or >2 g/dL below the LLN
- Bone lesions: >= 1 osteolytic lesion on imaging
- Biomarkers of malignancy
- > 60% clonal BM plasma cells
- Serum free-light-chain (SFLC) level >100 mg/L with an involved:uninvolved SFLC ratio >100
- >1 focal skeletal lesion on MRI (>5 mm in size)
- CRAB criteria (end-organ damage)
Serum/urine M(monoclonal) protein>3g/dL
BM plasmacytosis >10%
Bone scan, ALP – ????? ???
IVP? renal failure? ????? ??!
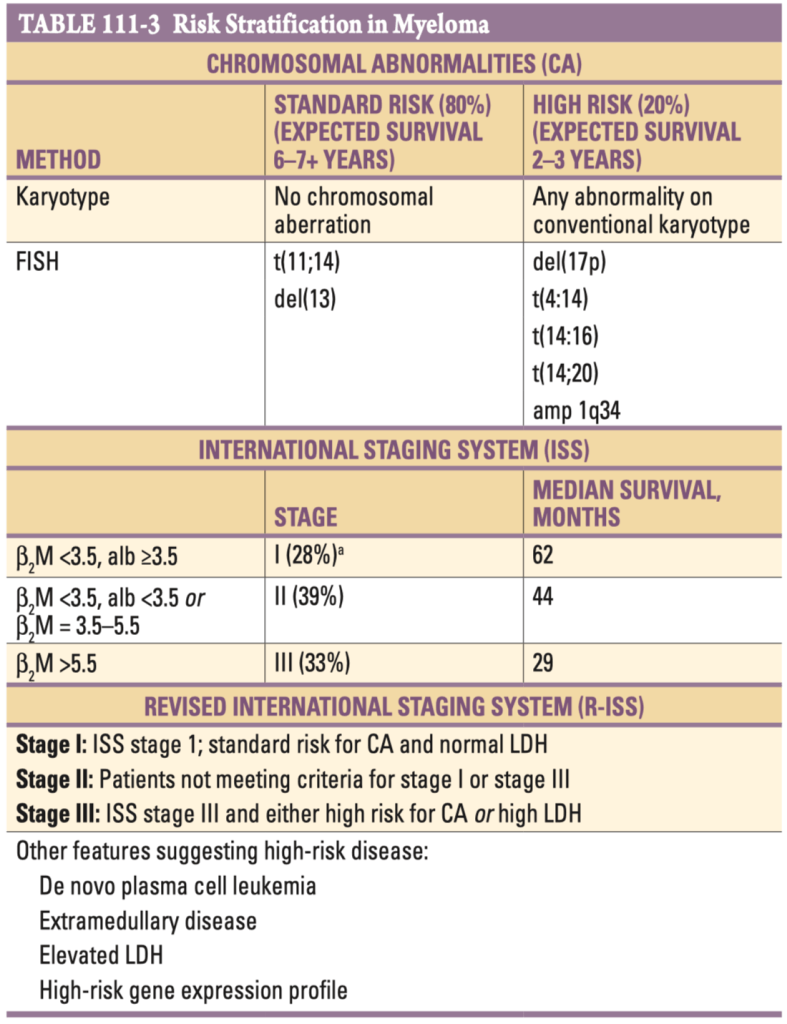
a: Percentage of patients presenting at each stage.
Abbreviations: β2 M, serum β2 -microglobulin in mg/L; alb, serum albumin in g/dL; FISH, fluorescent in situ hybridization; LDH, lactate dehydrogenase.
MGUS and SMM
Monoclonal gammopathy of undetermined significance (MGUS)
lncreased serum protein with M spike on SPEP; other features of multiple myeloma are absent (e.g., no lytic bone lesions, hypercalcemia, AL amyloid, or Bence Jones proteinuria).
Common in elderly (seen in 5% of 70-year-old individuals)
1% of patients with MGUS develop multiple myeloma each year.
Smoldering (asymptomatic) multiple myeloma (SMM)
May Clinic 2018 risk stratification for progression
- M protein >2g/dL
- BM clonal plasma cells >20%
- Involved-uninvolved free-light-chain ratio >20
-> 0: low risk / 1: intermediate risk / 2-3: high risk
Management
- MGUS and low- or intermediate-risk SMM
- Close observation (surveillance testing 2-3 months after initial diagnosis. Then 4-6 months for a year, then every 6-12 months.)
- High-risk SMM
- Considered for Lenalidomide + Dexamethasone
- Acute complications
- Plasmapheresis to remove lgM from the serum.
Prognosis
β2-microglobulin : single most powerful predictor of survival
Treatment

FIGURE 111-6 Treatment algorithm for multiple myeloma. C, cyclophosphamide; D, dexamethasone; M, melphalan; P, prednisone; R, lenalidomide; RVD-lite, weekly regimen; V, bortezomib. Alternate regimen indicates combinations including daratumumab, elotuzumab, panobinostat, carfilzomib, ixazomib, pomalidomide, or other agents. ASCT, autologous stem cell transplantation; HDT, high-dose therapy; MDE, myeloma-defining events.
- ???: ???? ??
- ?????? O (under 65 yo & good functional status)
- Induction CTx
- Velcade
- Thalidomide
- Dexamethasone
- ??? autologous BMT
- Induction CTx
- ???? ?? X (65~75?)
- Bortezomib + thalidomide + prednisone
- Salvage Tx: ??? ?? ??? ??? ??. Bortezomib or lenalidomide
- ??? ??
- Hypercalcemia: ????, bisphosphonate
- ??? ??: ?? ?? ??, UTI ?? ??
- Hyperviscosity: plasmapheresis
Complications
Renal disease
- Dysproteinemia-assoicated kidney disease
- Hypercalcemia-associated renal damage
- Analgesic nephropathy
Systemic disease
- AL amyloidosis
- Light chains can accumuluate as amyloids and may lead to restrictive cardiomyopathy, renal insufficiency, macrogloossia, and malabsorption syndromes
- Infections
- Secondary plasma cell leukemia
- Hypercalcemic crisis
Waldenström macroglobulinemia
B-cell lymphoma with monoclonal IgM production
Clinical features
- Generalized lymphadenopathy; lytic bone lesions are absent.
- Hyperviscosity syndrome
- Visual and neurologic deficits (e.g., retinal hemorrhage or stroke)
- Diplopia, tinnitus, headache, dilated/segmented funduscopic findings
- Bleeding: viscous serum results in defective platelet aggregation.
- Peripheral neuropathy
- Infiltrative disease
- Hypatosplenomegaly
- Anemia, thrombocytopenia
- Cryoglobulinemia
- Renal insufficiency
Physical exam
“Sausage-link” (dilated, segmented tortuous) retinal veins
Diagnosis
- SPEP
- If positive, BM biopsy