https://www.practicalradonc.org/article/S1879-8500(22)00273-9/fulltext
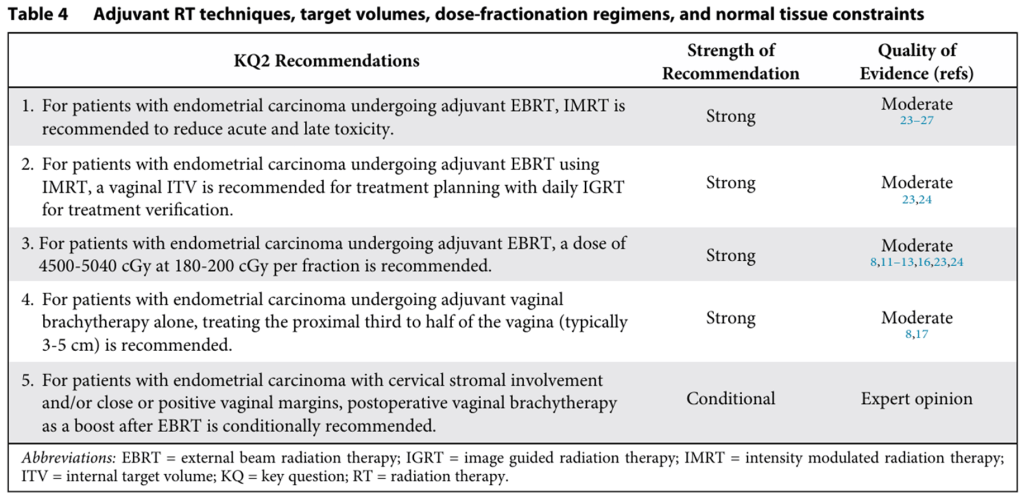
KQ1 : Adjuvant RT indication
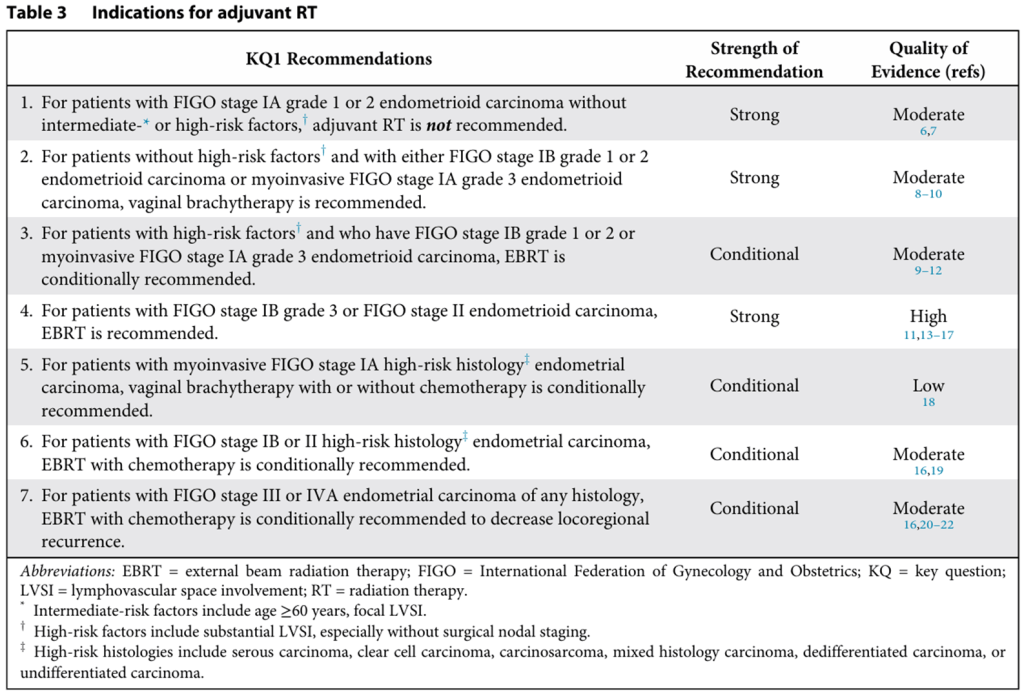
Stage I-II Endometrioid carcinoma
Figure 1 Stage I to II endometroid carcinoma.
*Intermediate-risk factors include age ≥60 years and focal LVSI. †High-risk factors include substantial LVSI, especially without surgical nodal staging.
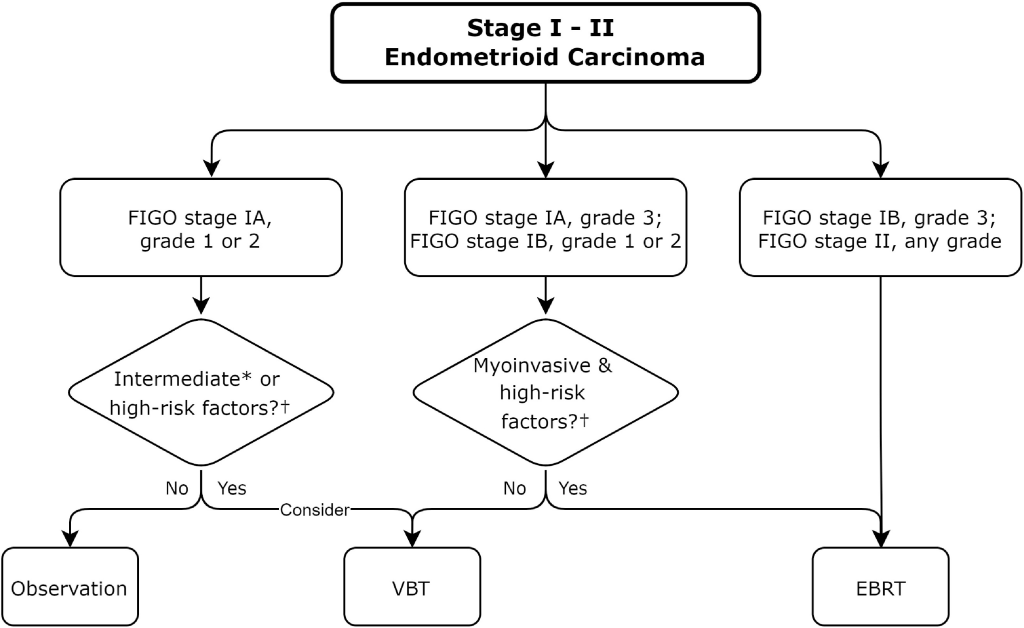
Stage I-II High-Risk Histologies
Figure 2 High-risk histologies.
*Serous carcinoma, clear cell carcinoma, carcinosarcoma, mixed histology carcinoma, dedifferentiated, or undifferentiated carcinoma.
†Molecular profiling may influence alternate treatment pathway selection.
Stage III-IVA (All Histologies)
GOG 122
- FIGO III-IVA, <2 cm of residual post-surgery
- WAI vs CTx alone (cisplatin+doxo)
Other 2 RCTs
- EBRT alone vs. CTx alone
- No difference in PFS or OS
PORTEC-III
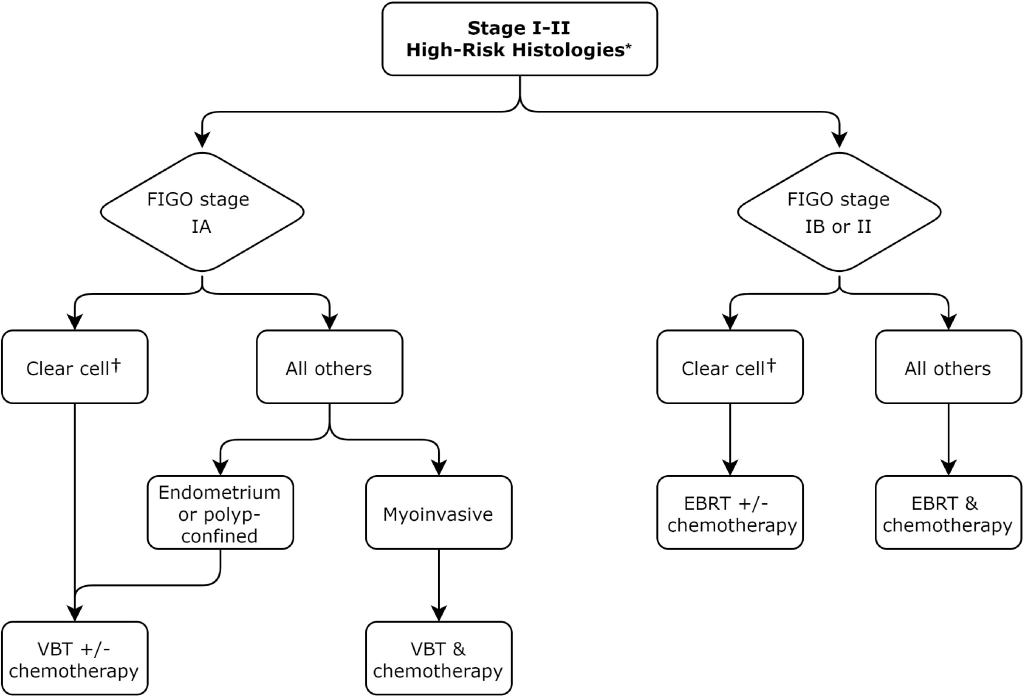
KQ2 : RT techniques, regimen
EBRT technique
- IMRT is strongly recommended
- RTOG 1203(TIME-C) demonstrated that IMRT (vs 3D-CRT) was associated with significantly lower rates of acute patient-reported GI, GU toxicity with improved QOL.
Targeting volume
- Vaginal ITV with daily IGRT is strongly recommended
- Vaginal ITV
- by merging scans taken with a full and an empty bladder.
- include vagina, residual parametria, and paravaginal tissues (if distended rectum, include anterior rectum in case of empty rectum)
- Daily Image Guided RT (IGRT): CBCT every day.
- Vaginal ITV
Dose fractionation (based on major prospective studies)
- The strongly recommended standard dose for adjuvant EBRT
- 4500–5040 cGy, delivered in daily fractions of 180–200 cGy to vaginal ITV
- EQD2 of 5500-6500cGy, either sequential or simultaneous to residual nodal diseases
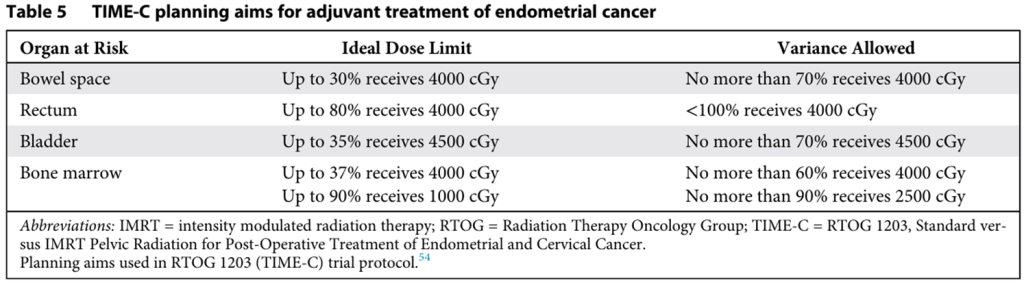
Normal Tissue Dose Limits
- Insufficient evidence to make formal recommendations
- RTOG 1203 (TIME-C) trial as “reasonable to follow”
Brachytherapy
- Traditional 6000-6500cGy LDR dose equivalent used.
- Contemporary lower dose regimens can be used.
- Refer to American Brachytherapy Society for more complete options
- Adj VBT Alone (Monotherapy)
- Strongly recommends treating the proximal third to half (3~5cm) of the vagina.
- The predominant location for recurrence. Treating the entire length of the vagina increases the risk of vaginal stenosis) (Retrospective analysis)
- -> LVSI or high-risk histology: longer length can be considered
- VBT Boost After EBRT
- Conditionally recommended in close or positive vaginal margins, cervical stromal involvement (With limited evidence)
KQ3 : Systemic therapy indication
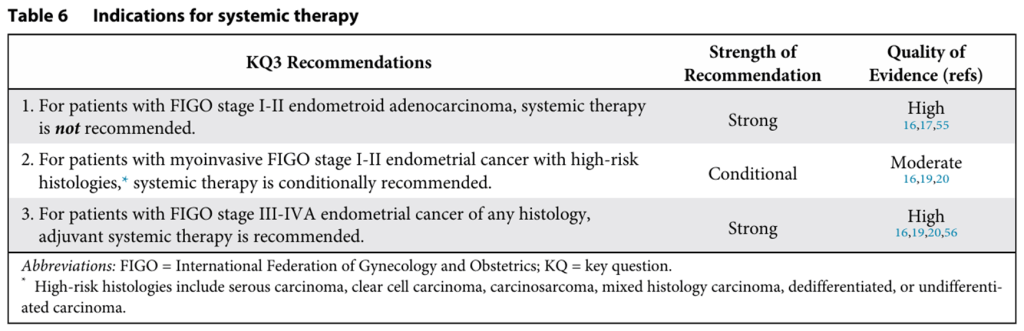
Stage I-II Endometrioid carcinoma
Systemic therapy is not recommended.
Stage I-II High-Risk Histologies
Systemic therapy is conditionally recommended
Stage III-IVA (All Histologies)
Systemic therapy is strongly recommended.
- GOG 122
- PORTEC-3
- GOG 258
KQ4 : Appropriate sequencing of systemic therapy with RT

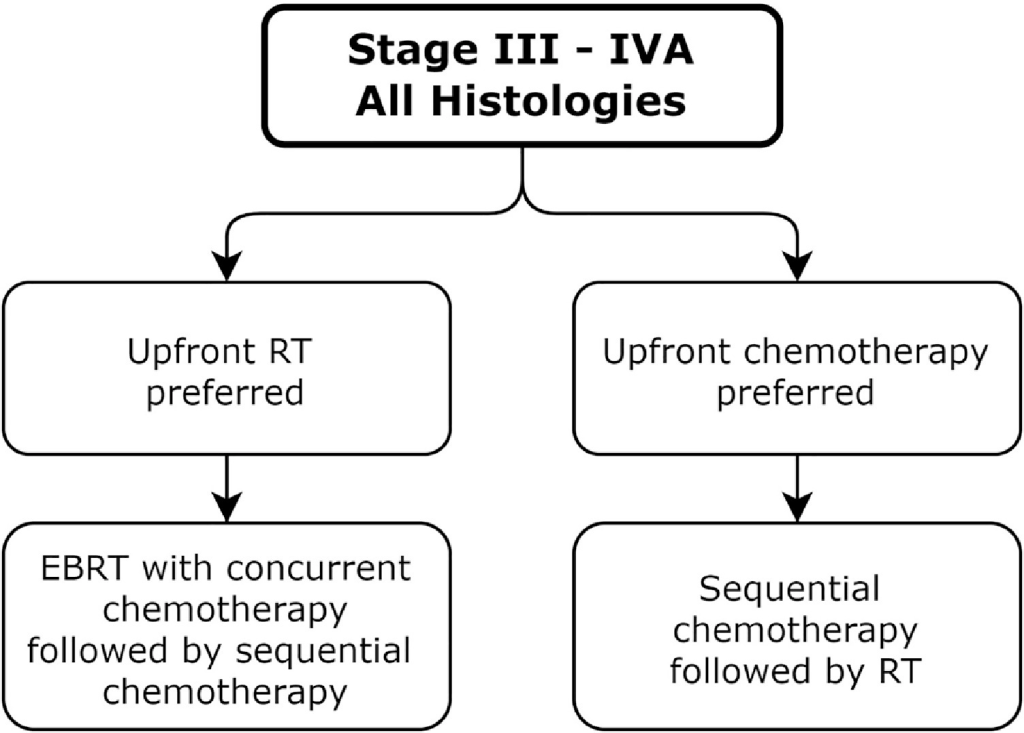
Stage III-IVA
Stage I-II with high-risk histologies
- For FIGO Stage I-II with High-Risk Histologies
- When both EBRT and chemotherapy are given, either sequential or concurrent treatment is strongly recommended. (as with PORTEC-3 and GOG 258 regimen)
- For Vaginal Brachytherapy (VBT) and Chemotherapy
- No RCT for optimal sequencing, but VBT is low-morbidity therapy: either sequential or concurrent treatment is strongly recommended.
- To avoid unnecessary risk, it is better not to administer VBT and chemotherapy on the same day
KQ5 : Adjuvant RT decisions based on LN assessment
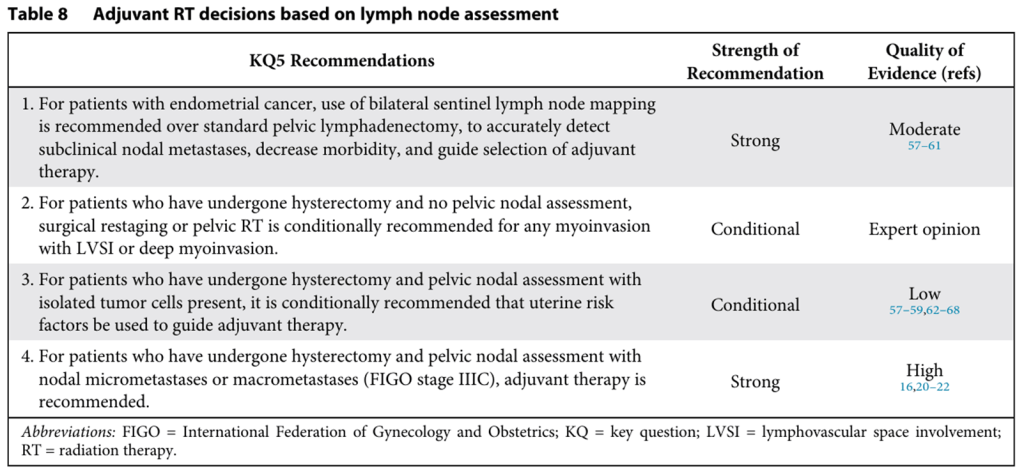
Bilateral sentinel lymph node (SLN) mapping is strongly recommended over standard pelvic lymphadenectomy. (Several retrospective and prospective studies (e.g. SENTOR))
- Increased Accuracy: Surgical precision by removing fewer but mor relevant nodes, more detailed analysis with “pathologic ultrastaging”
- Decreased Morbidity: Significantly lower rates of lower extremity lymphedema, compared to a full lymphadenectomy.
- Isolated Tumor Cells (ITC): <0.2mm or fewer than 200 cells found during ultrastaging -> pN0(i+), associated with other uterine risk factors but no prognostic value independantly
- Micrometastases: 0.2–2 mm or Macrometastases: >2 mm -> N+ -> stage IIIC
ITC
- Adjuvant therapy decisions is conditionally recommended based on uterine risk factors (like grade, histology, and LVSI), not on the presence of ITCs alone.
- Large center retrospective study shows that the prognosis for ITC is similar to node-negative patients. (Further verification of the importance of ITC is warranted.)
Micrometastases or Macrometastases
- Adjuvant therapy is strongly recommended.
- Multiple RTCs: micrometastases are associated with worse survival, which is improved with adjuvant therapy.
- Locoregional control important -> EBRT is recommended than chemo alone
No nodal assessment (Hysterectomy without nodal assessment)
- Surgical restaging or pelvic RT is conditionally recommended for patients with “any myoinvasion with LVSI or >50% myoinvasion“
- With an approximately 10% or greater risk of having positive lymph nodes
KQ6 : Adjuvant Therapy Decision
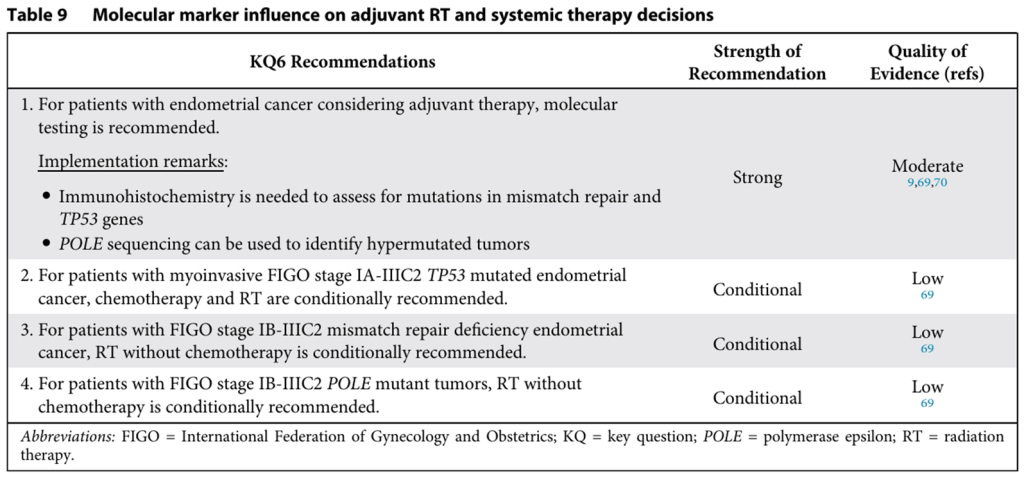
- This is one of the most significant updates in the guideline
- based on a molecular analysis of the PORTEC-3 trial, which originally compared EBRT alone vs. EBRT plus chemotherapy for high-risk endometrial cancer.
- Universal Testing using immunohistochemistry (IHC) to check for mismatch repair (MMR) proteins and p53, along with gene sequencing to identify POLE mutations
- Molecular testing is strongly recommended for patients with endometrial cancer who are considering adjuvant therapy
- The Cancer Genome Atlas (TCGA) classification (4 subsets identified)
- POLE ultramutated: Best prognosis.
- Mismatch Repair Deficient (MMR-d) or Microsatellite Instability Hypermutated (MSI-H): Intermediate prognosis.
- Copy Number Low or No Specific Molecular Profile (NSMP): Intermediate prognosis.
- Copy Number High (high rate of TP53 mutation (p53 abnormal)): Worst prognosis.
TP53 Mutated Tumors:
- Chemotherapy and RT are conditionally recommended.
- This was the only molecular subgroup in the PORTEC-3 trial that showed a significant and substantial benefit from the addition of chemotherapy. RT+Chemo (vs RT alone) improved the 5-year RFS from 36% to 59%.
MMR-d/MSI-H Tumors:
- RT without chemotherapy is conditionally recommended.
- The PORTEC-3 analysis showed no difference in 5yr RFS for MMR-d patients.
- May be treated with adjuvant immunotherapy (NRG-GY020 ongoing).
POLE Mutant Tumors:
- RT without chemotherapy is conditionally recommended.
- Excellent prognosis: PORTEC-3 study, only 1 out of 51 patients (EBRT only) had a disease recurrence.
- Single modality (RT only) may be sufficient. Ongoing trials of eliminating adjuvant therapy (PORTEC-4a, TAPER)